

Biomechanical engineering comparison of four leaflet repair techniques for mitral regurgitation using a novel 3-dimensional-printed left heart simulator
- PMID: 34977730
- PMCID: PMC8691825
- DOI: 10.1016/j.xjtc.2021.09.040
Biomechanical engineering comparison of four leaflet repair techniques for mitral regurgitation using a novel 3-dimensional-printed left heart simulator
Abstract
Objective: Mitral valve repair is the gold standard treatment for degenerative mitral regurgitation; however, a multitude of repair techniques exist with little quantitative data comparing these approaches. Using a novel ex vivo model, we sought to evaluate biomechanical differences between repair techniques.
Methods: Using porcine mitral valves mounted within a custom 3-dimensional-printed left heart simulator, we induced mitral regurgitation using an isolated P2 prolapse model by cutting primary chordae. Next, we repaired the valves in series using the edge-to-edge technique, neochordoplasty, nonresectional remodeling, and classic leaflet resection. Hemodynamic data and chordae forces were measured and analyzed using an incomplete counterbalanced repeated measures design with the healthy pre-prolapse valve as a control.
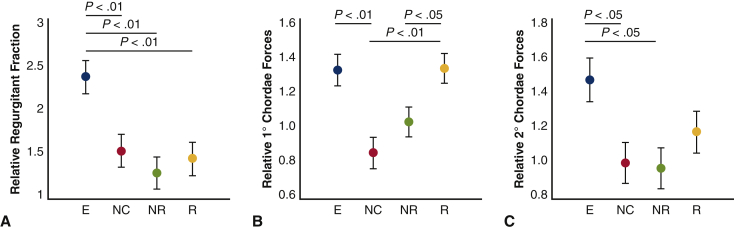
Results: With the exception of the edge-to-edge technique, all repair methods effectively corrected mitral regurgitation, returning regurgitant fraction to baseline levels (baseline 11.9% ± 3.7%, edge-to-edge 22.5% ± 6.9%, nonresectional remodeling 12.3% ± 3.0%, neochordal 13.4% ± 4.8%, resection 14.7% ± 5.5%, P < 0.01). Forces on the primary chordae were minimized using the neochordal and nonresectional techniques whereas the edge-to-edge and resectional techniques resulted in significantly elevated primary forces. Secondary chordae forces also followed this pattern, with edge-to-edge repair generating significantly higher secondary forces and leaflet resection trending higher than the nonresectional and neochord repairs.
Conclusions: Although multiple methods of degenerative mitral valve repair are used clinically, their biomechanical properties vary significantly. Nonresectional techniques, including leaflet remodeling and neochordal techniques, appear to result in lower chordal forces in this ex vivo technical engineering model.
Keywords: 3D, 3-dimensional; FBG, Fiber Bragg Grating; MR, mitral regurgitation; biomechanics; chordae forces; ex vivo model; leaflet remodeling; leaflet resection; mitral valve repair; neochord.
© 2021 The Author(s).
Figures




Comment in
-
Commentary: Biomechanical differences after mitral valve repair: Is it time to use the science?JTCVS Tech. 2021 Oct 26;10:252-253. doi: 10.1016/j.xjtc.2021.10.042. eCollection 2021 Dec. JTCVS Tech. 2021. PMID: 34984385 Free PMC article. No abstract available.
References
-
- Devereux R.B., Jones E.C., Roman M.J., Howard B.V., Fabsitz R.R., Liu J.E., et al. Prevalence and correlates of mitral valve prolapse in a population-based sample of American Indians: the Strong Heart Study. Am J Med. 2001;111:679–685. - PubMed
-
- Freed L.A., Levy D., Levine R.A., Larson M.G., Evans J.C., Fuller D.L., et al. Prevalence and clinical outcome of mitral-valve prolapse. N Engl J Med. 1999;341:1–7. - PubMed
-
- de Marchena E., Badiye A., Robalino G., Junttila J., Atapattu S., Nakamura M., et al. Respective prevalence of the different carpentier classes of mitral regurgitation: a stepping stone for future therapeutic research and development. J Card Surg. 2011;26:385–392. - PubMed
-
- Hayek E., Gring C.N., Griffin B.P. Mitral valve prolapse. Lancet. 2005;365:507–518. - PubMed
-
- Mozaffarian D., Benjamin E.J., Go A.S., Arnett D.K., Blaha M.J., Cushman M., et al. Heart disease and stroke statistics–2015 update: a report from the American Heart Association. Circulation. 2015;131:e29–e322. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
