

Quality of facility-based maternal and newborn care around the time of childbirth during the COVID-19 pandemic: online survey investigating maternal perspectives in 12 countries of the WHO European Region
- PMID: 34977838
- PMCID: PMC8703114
- DOI: 10.1016/j.lanepe.2021.100268
Quality of facility-based maternal and newborn care around the time of childbirth during the COVID-19 pandemic: online survey investigating maternal perspectives in 12 countries of the WHO European Region
Erratum in
-
Corrections to "Quality of facility-based maternal and newborn care around the time of childbirth during the COVID-19 pandemic: Online survey investigating maternal perspectives in 12 countries of the WHO European Region".Lancet Reg Health Eur. 2022 Jul 22;19:100461. doi: 10.1016/j.lanepe.2022.100461. eCollection 2022 Aug. Lancet Reg Health Eur. 2022. PMID: 35891895 Free PMC article.
Abstract
Background: Multi-country studies assessing the quality of maternal and newborn care (QMNC) during the COVID-19 pandemic, as defined by WHO Standards, are lacking.
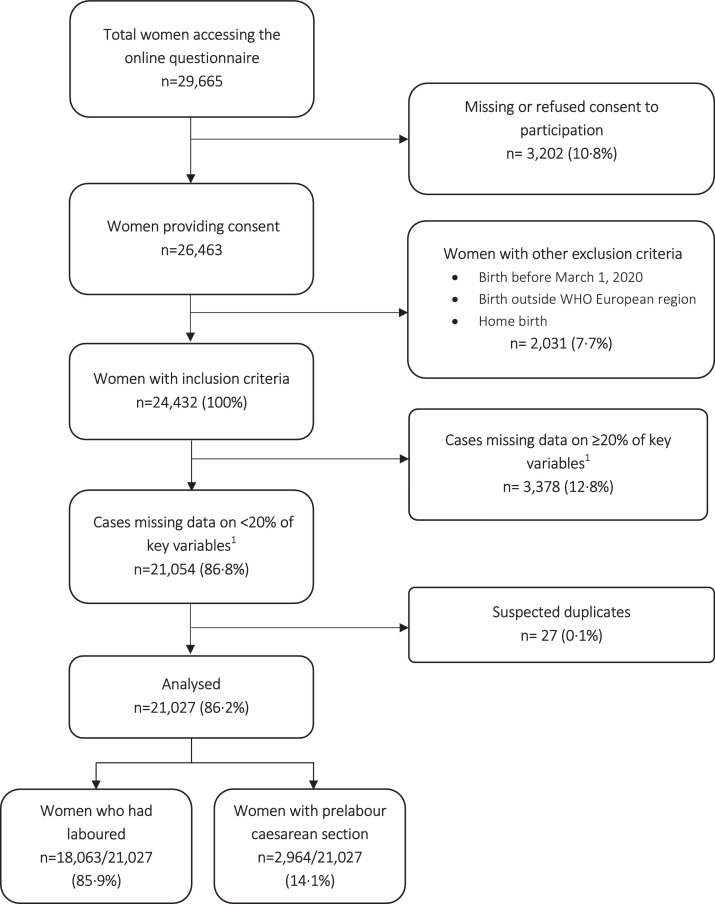
Methods: Women who gave birth in 12 countries of the WHO European Region from March 1, 2020 - March 15, 2021 answered an online questionnaire, including 40 WHO Standard-based Quality Measures.
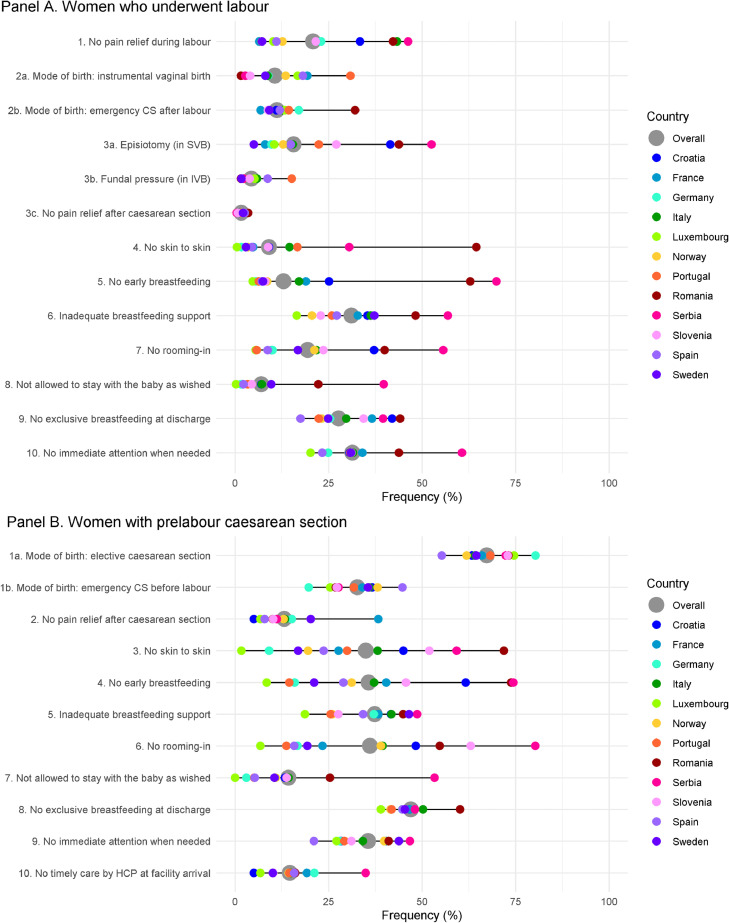
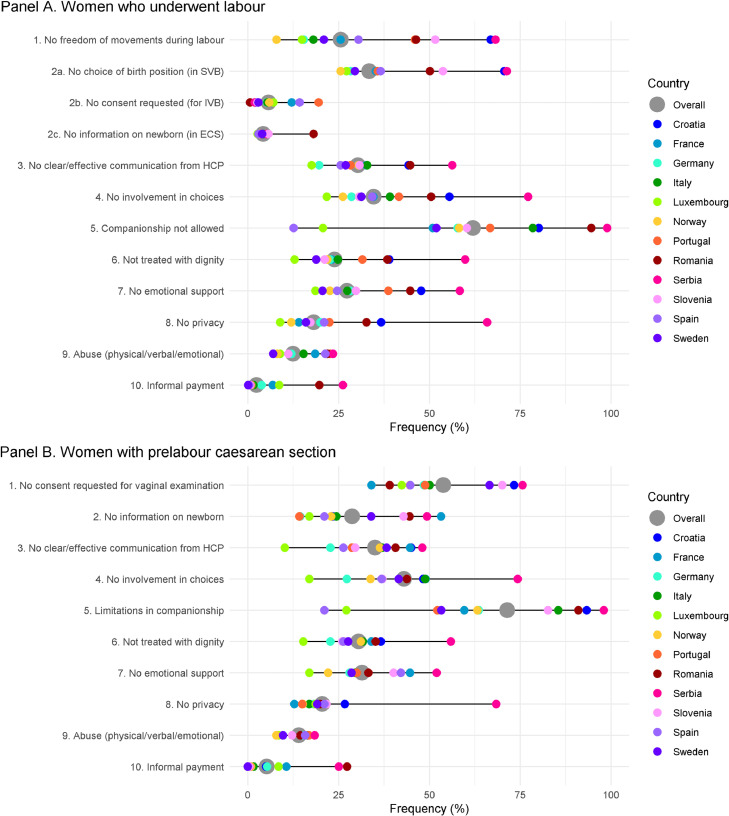
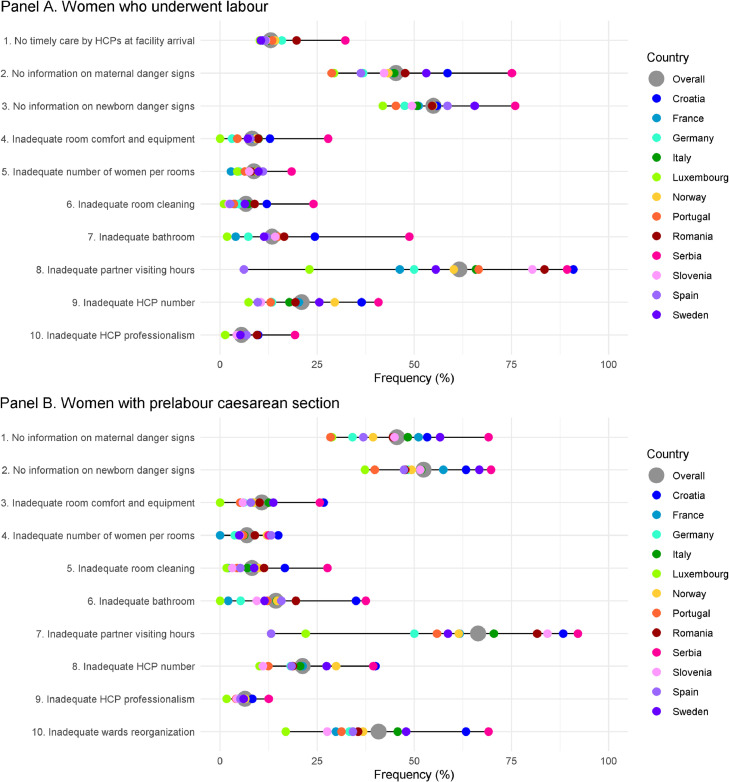
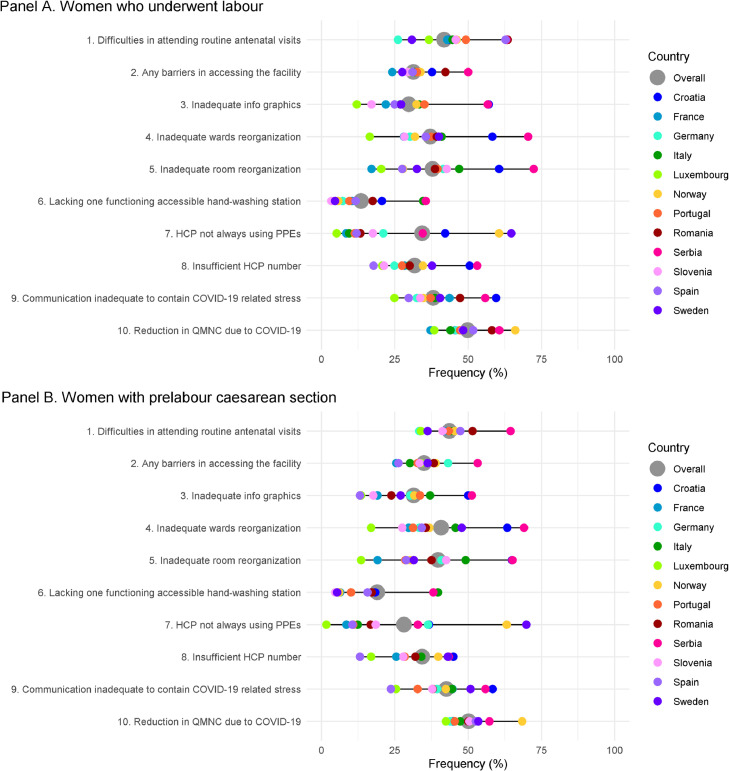
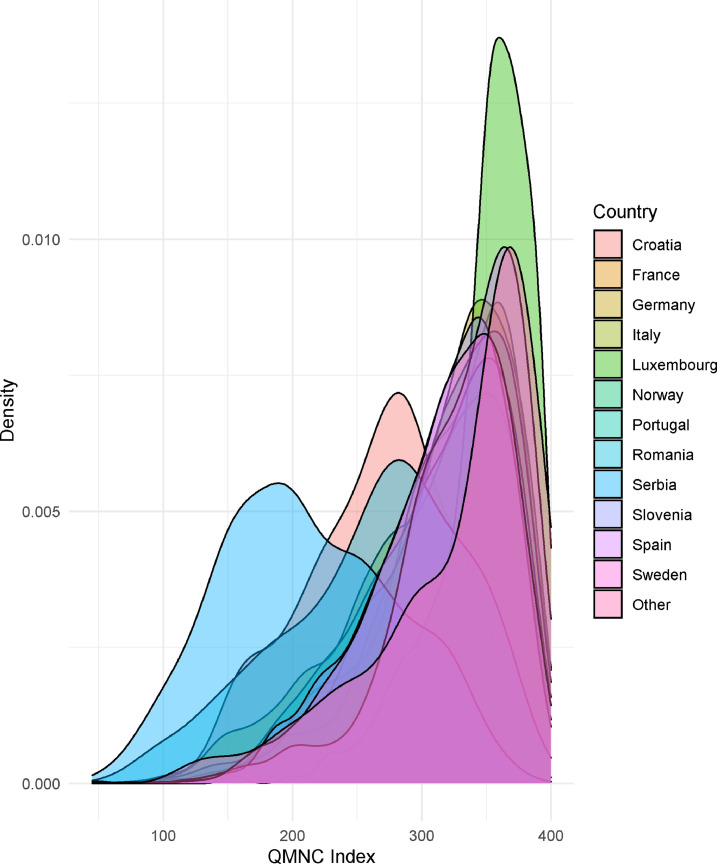
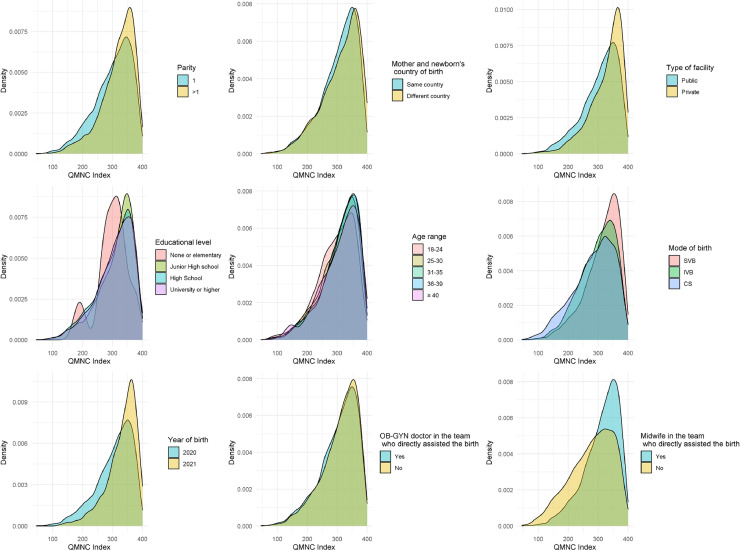
Findings: 21,027 mothers were included in the analysis. Among those who experienced labour (N=18,063), 41·8% (26·1%- 63·5%) experienced difficulties in accessing antenatal care, 62% (12·6%-99·0%) were not allowed a companion of choice, 31·1% (16·5%-56·9%) received inadequate breastfeeding support, 34·4% (5·2%-64·8%) reported that health workers were not always using protective personal equipment, and 31·8% (17·8%-53·1%) rated the health workers' number as "insufficient". Episiotomy was performed in 20·1% (6·1%-66·0%) of spontaneous vaginal births and fundal pressure applied in 41·2% (11·5% -100%) of instrumental vaginal births. In addition, 23·9% women felt they were not treated with dignity (12·8%-59·8%), 12·5% (7·0%-23·4%) suffered abuse, and 2·4% (0·1%-26·2%) made informal payments. Most findings were significantly worse among women with prelabour caesarean birth (N=2,964). Multivariate analyses confirmed significant differences among countries, with Croatia, Romania, Serbia showing significant lower QMNC Indexes and Luxemburg showing a significantly higher QMNC Index than the total sample. Younger women and those with operative births also reported significantly lower QMNC Indexes.
Interpretation: Mothers reports revealed large inequities in QMNC across countries of the WHO European Region. Quality improvement initiatives to reduce these inequities and promote evidence-based, patient-centred respectful care for all mothers and newborns during the COVID-19 pandemic and beyond are urgently needed.
Funding: The study was financially supported by the Institute for Maternal and Child Health IRCCS Burlo Garofolo, Trieste, Italy.
Study registration: ClinicalTrials.gov Identifier: NCT04847336.
Keywords: COVID-19; European Region; WHO; facility; maternal; newborn; quality of care; questionnaire; respectful maternity care; survey.
© 2021 The Author(s).
Conflict of interest statement
Céline Miani's position as a post-doctoral researcher is funded by Bielefeld University. Catarina Barata had a PhD grant FCT/FSE (SFRH/BD/128600/2017) while she was voluntarily writing this article. She is board member, unpaid collaboration, of Associação Portuguesa pelos Direitos da Mulher na Gravidez e Parto (APDMGP). Daniela Drandić received a salary during the time she was volunteer-writing this article was from a grant from the Erasmus+ programme of the European Commission, regarding a project on parenting support and from a grant from the UNICEF Croatia, regarding a project on online education for pregnant women during COVID. She is a board member of an NGO called Human Rights in Childbirth, and has been for the entire time she worked on this paper. Dr Emma Sacks has received research funding from the World Health Organization related to the mistreatment of women and newborns in health facilities. The project has no impact on the present manuscript outside of similar topics. She is the former co-chair of the Newborn Health Working Group of the Global Respectful Maternity Care Council. Other authors have none to declare.
Figures
Comment in
-
IMAgiNE EURO: Data for action on quality of maternal and newborn care in 20 European countries during the COVID-19 pandemic.Int J Gynaecol Obstet. 2022 Dec;159 Suppl 1(Suppl 1):5-8. doi: 10.1002/ijgo.14500. Int J Gynaecol Obstet. 2022. PMID: 36530004 Free PMC article.
References
-
- Chmielewska B, Barratt I, Townsend R, Kalafat E, van der Meulen J, Gurol-Urganci I, O'Brien P, Morris E, Draycott T, Thangaratinam S, Le Doare K, Ladhani S, von Dadelszen P, Magee L, Khalil A. Effects of the COVID-19 pandemic on maternal and perinatal outcomes: a systematic review and meta-analysis. Lancet Glob Health. 2021 S2214-109X(21)00079-6. - PMC - PubMed
-
- Kc A, Gurung R, Kinney MV, Sunny AK, Moinuddin M, Basnet O, Paudel P, Bhattarai P, Subedi K, Shrestha MP, Lawn JE, Målqvist M. Effect of the COVID-19 pandemic response on intrapartum care, stillbirth, and neonatal mortality outcomes in Nepal: a prospective observational study. Lancet Glob Health. 2020;8(10):e1273–e1281. - PMC - PubMed
-
- Ceulemans M, Verbakel JY, Van Calsteren K, Eerdekens A, Allegaert K, Foulon V. SARS-CoV-2 Infections and Impact of the COVID-19 Pandemic in Pregnancy and Breastfeeding: Results from an Observational Study in Primary Care in Belgium. Int J Environ Res Public Health. 2020;17(18):6766. doi: 10.3390/ijerph17186766. - DOI - PMC - PubMed
-
- Naurin E, Markstedt E, Stolle D, Enström D, Wallin A, Andreasson I, Attebo B, Eriksson O, Martinsson K, Elden H, Linden K, Sengpiel V. Pregnant under the pressure of a pandemic: a large-scale longitudinal survey before and during the COVID-19 outbreak. Eur J Public Health. 2021;31(1):7–13. 6000. - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
