

Mucormycosis: A triple burden in patients with diabetes during COVID-19 Pandemic
- PMID: 34977914
- PMCID: PMC8639489
- DOI: 10.1016/j.hsr.2021.100005
Mucormycosis: A triple burden in patients with diabetes during COVID-19 Pandemic
Abstract
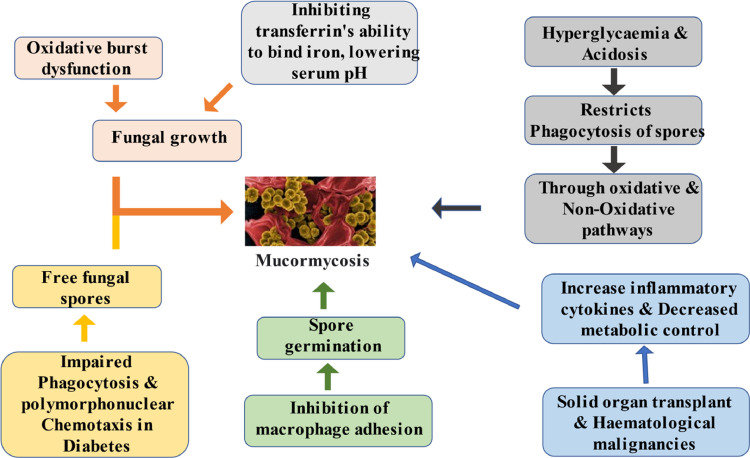
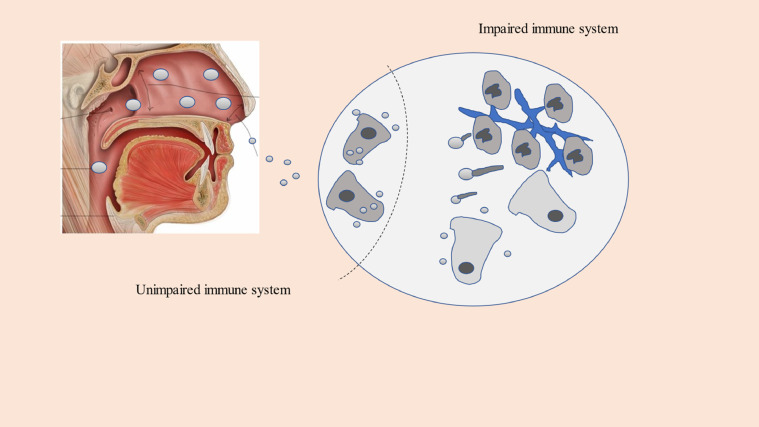
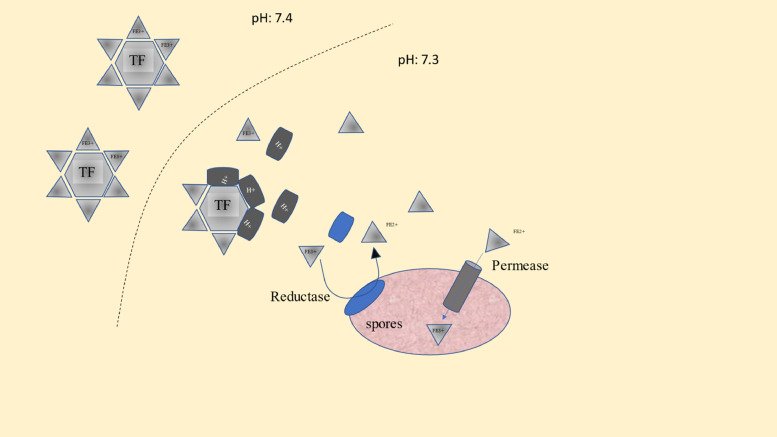
With the upsurge in the cases of COVID-19 around the world, plenty of potential COVID-19 complications are becoming more prevalent, including a higher risk of secondary bacterial and fungal infections. Mucormycosis is one such condition which has high prevalence among individuals with diabetes who were infected with COVID-19.The usage of steroids in the treatment further inflates the risk of infection and exacerbation of disease in pre-existent mucormycosis patients. Generally, Corticosteroid-induced diabetes can arise on long-term steroid medication, increasing the likelihood of mucormycosis. In patients with COVID-19, the indications and dose of corticosteroids should be properly regulated, and persons with diabetes who take insulin or oral anti-diabetic medicines should be cautious. To avoid poor outcomes, strategies to improve glycemic management should be emphasized. This narrative review elucidates different disciplines on rampant use of steroids, iron and zinc supplements as well as the methods utilized as primary or adjunctive treatment of this fatal condition. This article may help to pave the way for robust research that needs to be done to tackle the deadly triple burden of the disease.
Keywords: COVID-19; Diabetes; Mucormycosis; Triple burden.
© 2021 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
-
- Moorthy A., Gaikwad R., Krishna S., Hegde R., Tripathi K.K., Kale P.G., Rao P.S., Haldipur D., Bonanthaya K. SARS-CoV-2, uncontrolled diabetes and corticosteroids—an unholy trinity in invasive fungal infections of the maxillofacial region? A retrospective, multi-centric analysis. J. Maxillofac. Oral Surg. 2021:1–8. doi: 10.1007/s12663-021-01532-1. Mar 6. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources