

Role of progenitor cell marker CD133 in supporting diagnosis of collapsing glomerulopathy
- PMID: 34978023
- PMCID: PMC8720538
- DOI: 10.1007/s11255-021-03078-0
Role of progenitor cell marker CD133 in supporting diagnosis of collapsing glomerulopathy
Abstract
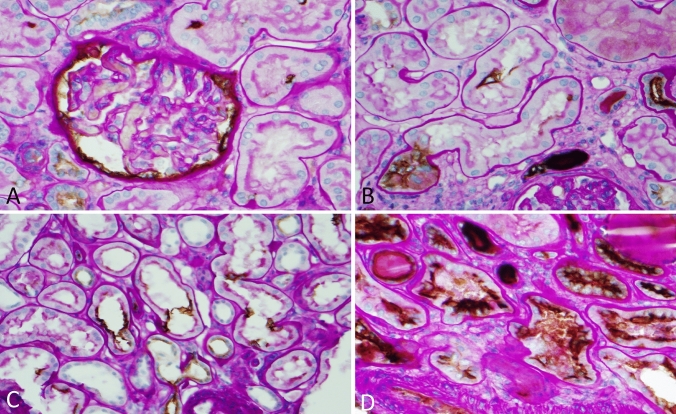
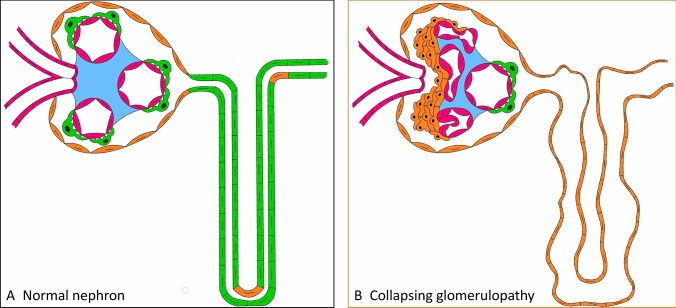
Purpose: A previous immunofluorescent study suggests that, in collapsing glomerulopathy, most hyperplastic podocytes that stained positively for a progenitor cell marker CD133 are derived from CD133 + parietal epithelial cells. In pathology practice, not all renal biopsies with collapsing glomerulopathy show the typical morphologic features for this entity, which include florid podocyte hyperplasia, collapsing glomerular capillary loops, and cystic tubular dilation. This study was made to determine if CD133 staining using an immunohistochemical method can be used to confirm hyperplastic podocytes and identify extensive acute tubular injury in collapsing glomerulopathy.
Methods: Twenty-one collapsing glomerulopathy biopsies were stained for CD133 and compared with 15 biopsies with focal segmental glomerulosclerosis, not otherwise specified (FSGS).
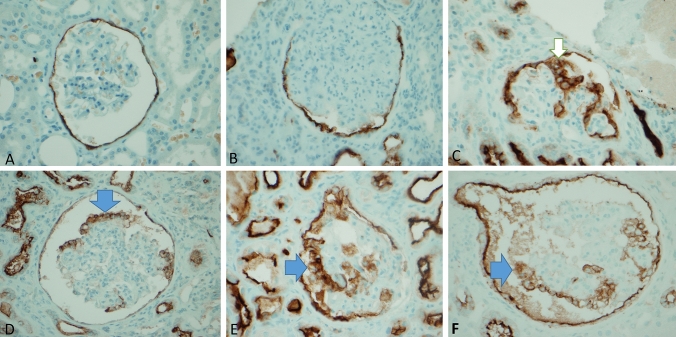
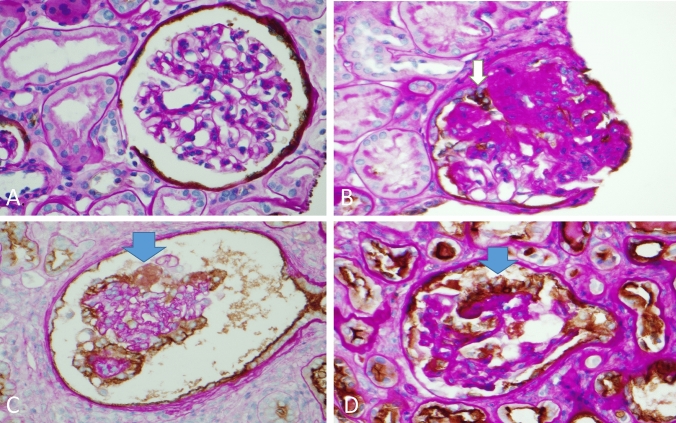
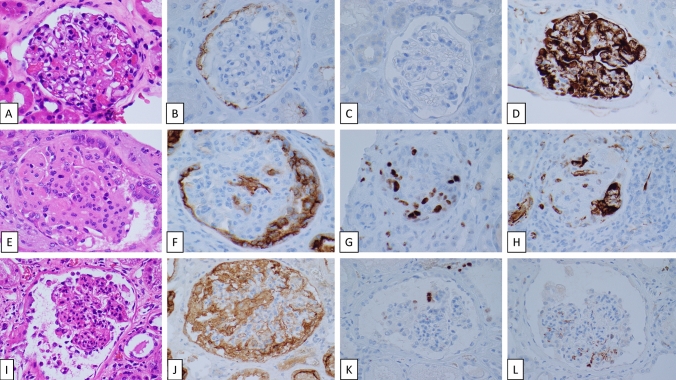
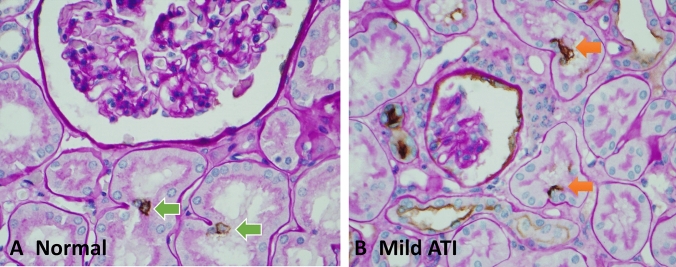
Results: All patients with collapsing glomerulopathy were of African American descent with prominent renal failure and nephrotic range proteinuria. In contrast, the FSGS group consisted of patients from a variety of ethnic backgrounds with nephrotic range proteinuria but relatively low serum creatinine. The striking finding was that all collapsing glomerulopathy cases showed positive CD133 staining in the clusters of hyperplastic podocytes. There was significantly higher CD133-positive staining rate for hyperplastic podocytes (38%) in the glomeruli of the collapsing glomerulopathy group when compared to small clusters of hyperplastic podocytes in the FSGS group (8%). In addition, when compared to the relatively weak CD133 staining in the proximal tubules of the FSGS group, the proximal tubules of the collapsing glomerulopathy group all showed diffuse and strong CD133 staining as a feature of severe acute tubular injury, which corresponded to the high serum creatinine levels in these patients.
Conclusion: Our data indicate that the combination of the distinctive mosaic CD133 staining in hyperplastic podocytes and the diffuse tubular CD133 staining is helpful in supporting a diagnosis of collapsing glomerulopathy.
Keywords: Acute tubular injury; CD133; Collapsing glomerulopathy; Focal segmental glomerulosclerosis; Parietal epithelium; Progenitor cells; Proliferative podocytes.
© 2021. The Author(s), under exclusive licence to Springer Nature B.V.
Conflict of interest statement
AYX declares that he has no conflict of interest. HDK declares that he has no conflict of interest. ZL declares that he has no conflict of interest. WL declares that she has no conflict of interest. PLZ declares that he has no conflict of interest.
Figures
Similar articles
-
Collapsing glomerulopathy: a clinically and pathologically distinct variant of focal segmental glomerulosclerosis.Kidney Int. 1994 May;45(5):1416-24. doi: 10.1038/ki.1994.185. Kidney Int. 1994. PMID: 8072254
-
Collapsing glomerulopathy: clinical characteristics and follow-up.Am J Kidney Dis. 1999 Apr;33(4):652-7. doi: 10.1016/s0272-6386(99)70215-5. Am J Kidney Dis. 1999. PMID: 10196005
-
HIV-associated nephropathy: experimental models.Contrib Nephrol. 2011;169:270-285. doi: 10.1159/000320212. Epub 2011 Jan 20. Contrib Nephrol. 2011. PMID: 21252526
-
Collapsing glomerulopathy: unraveling varied pathogeneses.Curr Opin Nephrol Hypertens. 2023 May 1;32(3):213-222. doi: 10.1097/MNH.0000000000000873. Epub 2023 Feb 9. Curr Opin Nephrol Hypertens. 2023. PMID: 36811644 Review.
-
Collapsing glomerulopathy.Semin Nephrol. 2003 Mar;23(2):209-18. doi: 10.1053/snep.2003.50019. Semin Nephrol. 2003. PMID: 12704581 Review.
Cited by
-
How Stem and Progenitor Cells Can Affect Renal Diseases.Cells. 2024 Aug 30;13(17):1460. doi: 10.3390/cells13171460. Cells. 2024. PMID: 39273032 Free PMC article. Review.
References
-
- Katoh Y, Katoh M. Comparative genomics on PROM1 gene encoding stem cell marker CD133. Int J Mol Med. 2007;19(6):967–970. - PubMed
-
- Sagrinati C, Netti GS, Mazzinghi B, Lazzeri E, Liotta F, Frosali F, Ronconi E, Meini C, Gacci M, Squecco R, Carini M, Gesualdo L, Francini F, Maggi E, Annunziato F, Lasagni L, Serio M, Romagnani S, Romagnani P. Isolation and characterization of multipotent progenitor cells from the Bowman’s capsule of adult human kidneys. J Am Soc Nephrol. 2006;17(9):2443–2456. doi: 10.1681/ASN.2006010089. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
