

Anatomical variation of inner ear may be a predisposing factor for unilateral Ménière's disease rather than for ipsilateral delayed endolymphatic hydrops
- PMID: 34978581
- PMCID: PMC9038801
- DOI: 10.1007/s00330-021-08430-7
Anatomical variation of inner ear may be a predisposing factor for unilateral Ménière's disease rather than for ipsilateral delayed endolymphatic hydrops
Abstract
Objective: Radiological anatomical variations, measured by magnetic resonance imaging (MRI), were evaluated in patients with ipsilateral delayed endolymphatic hydrops (DEH) and unilateral Ménière's disease (MD). The role of anatomical variations in different subtypes of hydropic ear disease was investigated.
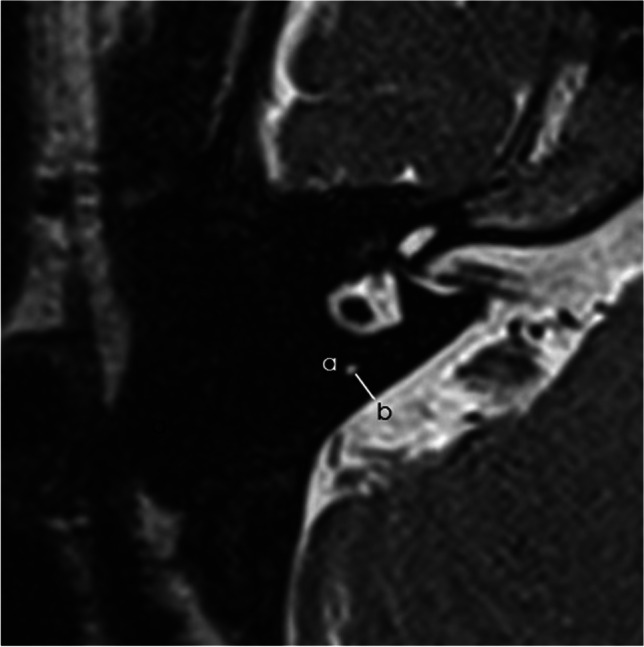
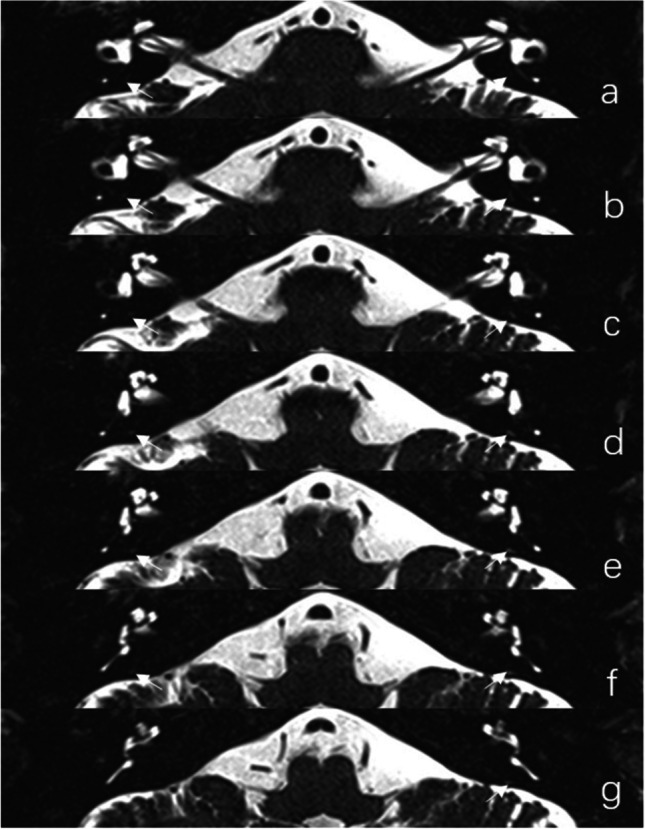
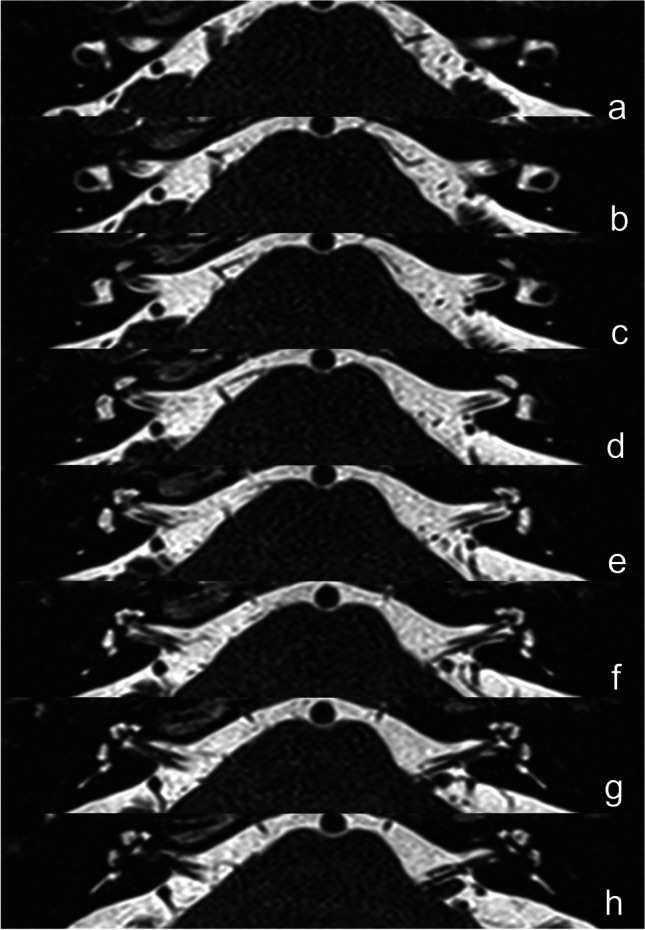
Methods: Twenty-eight patients with ipsilateral DEH, 76 patients with unilateral MD, and 59 control subjects were enrolled. The radiological indices included the distance between the vertical part of the posterior semicircular canal and the posterior fossa (MRI-PP distance) and the visibility of vestibular aqueduct (MRI-VA). These variations among patients with DEH, MD, and control subjects were compared. The correlation between radiological anatomical variations and clinical features or audio-vestibular findings was also examined.
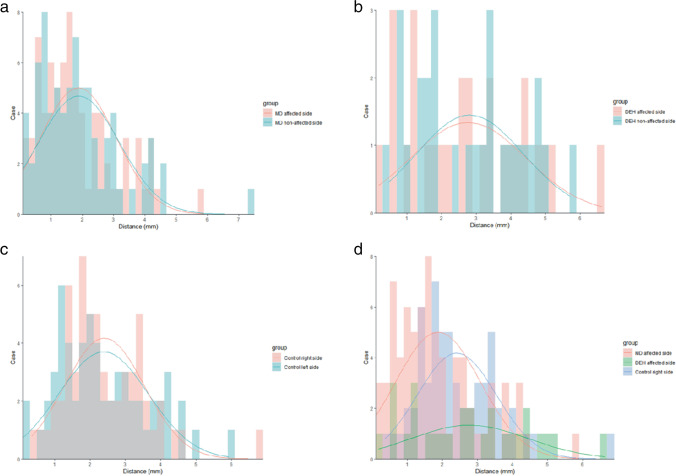
Results: (1) MRI-PP distance in the affected side of unilateral MD was shorter than that in ipsilateral DEH (Z = - 2.481, p = 0.013) and control subjects (Z = - 2.983, p = 0.003), while the difference of MRI-PP distance between the affected side of ipsilateral DEH and control subjects was not statistically significant (Z = - 0.859, p = 0.391). (2) There was no significant interaural difference of MRI-PP distance in patients with unilateral MD (Z = - 0.041, p = 0.968) and ipsilateral DEH (t = - 0.107, p = 0.915) respectively. (3) No significant interaural difference of MRI-VA visibility was observed in patients with unilateral MD (χ2 = 0.742, p = 0.389) and ipsilateral DEH (χ2 = 0.327, p = 0.567) respectively. (4) No correlation was found between these anatomical variables and clinical features or audio-vestibular findings in patients with unilateral MD and ipsilateral DEH respectively (p > 0.05).
Conclusions: Anatomical variations of inner ear may be a predisposing factor in the pathogenesis of unilateral MD rather than ipsilateral DEH.
Key points: • Patients with ipsilateral delayed endolymphatic hydrops showed normal distance between the vertical part of the posterior semicircular canal and the posterior fossa. • Compared to patients with ipsilateral delayed endolymphatic hydrops and control subjects, patients with unilateral Ménière's disease exhibited shorter distance between the vertical part of the posterior semicircular canal and the posterior fossa. • Anatomical variations of inner ear may be a predisposing factor in the pathogenesis of unilateral Ménière's disease rather than ipsilateral delayed endolymphatic hydrops.
Keywords: Endolymphatic hydrops; Endolymphatic sac; Magnetic resonance imaging; Ménière’s disease.
© 2021. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
References
-
- Mateijsen DJ, Van Hengel PW, Krikke AP, Van Huffelen WM, Wit HP, Albers FW. Three-dimensional Fourier transformation constructive interference in steady state magnetic resonance imaging of the inner ear in patients with unilateral and bilateral Meniere's disease. Otol Neurotol. 2002;23:208–213. doi: 10.1097/00129492-200203000-00017. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
