

Association of left atrial strain by cardiovascular magnetic resonance with recurrence of atrial fibrillation following catheter ablation
- PMID: 34980165
- PMCID: PMC8722067
- DOI: 10.1186/s12968-021-00831-3
Association of left atrial strain by cardiovascular magnetic resonance with recurrence of atrial fibrillation following catheter ablation
Abstract
Background: Atrial fibrillation (AF) is a progressive condition, which is characterized by inflammation/fibrosis of left atrial (LA) wall, an increase in the LA size/volumes, and decrease in LA function. We sought to investigate the relationship of anatomical and functional parameters obtained by cardiovascular magnetic resonance (CMR), with AF recurrence in paroxysmal AF (pAF) patients after catheter ablation.
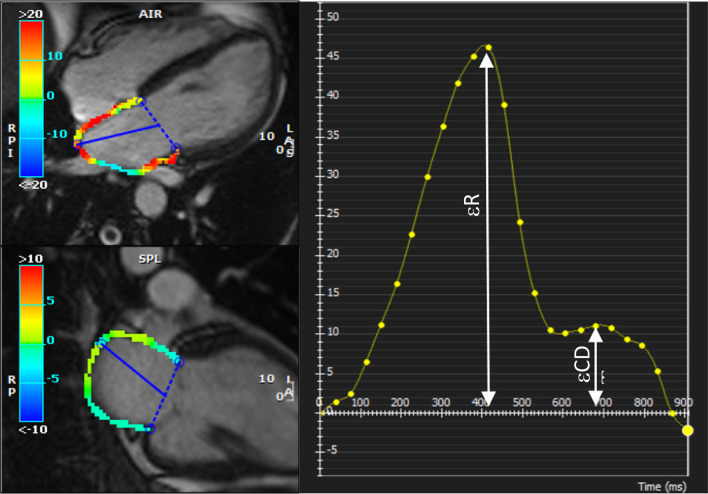
Methods: We studied 80 consecutive pAF patients referred for ablation, between January 2014 and December 2019, who underwent pre- and post-ablation CMR while in sinus rhythm. LA volumes were measured using the area-length method and included maximum, minimum, and pre-atrial-contraction volumes. CMR-derived LA reservoir strain (ℇR), conduit strain (ℇCD), and contractile strain (ℇCT) were measured by computer assisted manual planimetry. We used a multivariate logistical regression to estimate the independent predictors of AF recurrence after ablation.
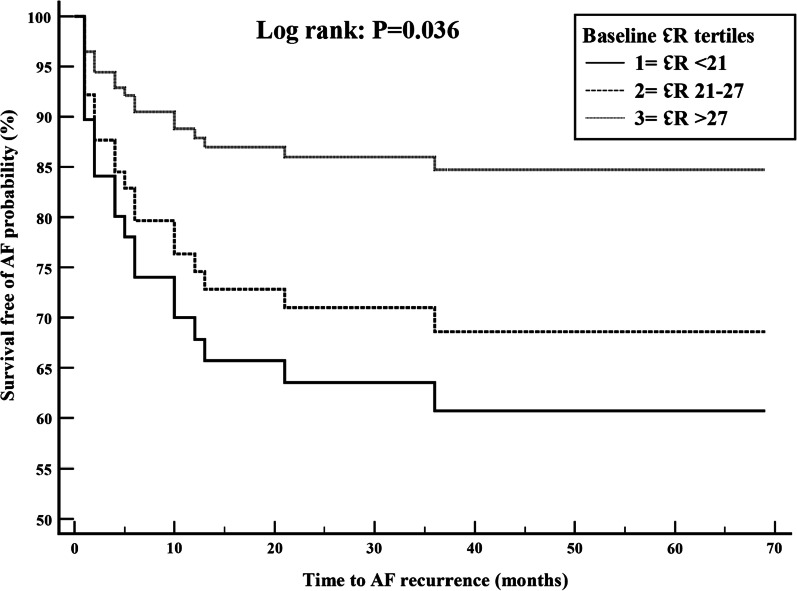
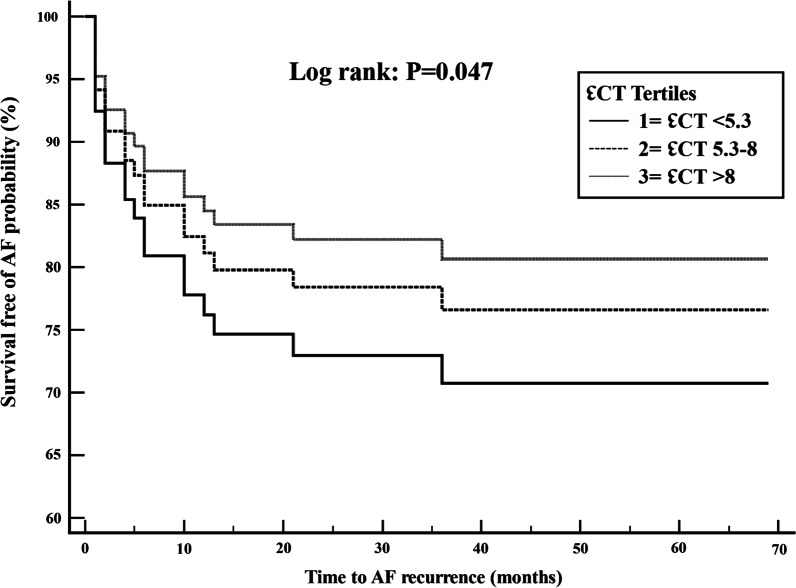
Results: Mean age was 58.6 ± 9.4 years, 75% men, mean CHA2DS2-VASc score was 1.7, 36% had prior cardioversion and 51% were taking antiarrhythmic drugs. Patients were followed for a median of 4 years (Q1-Q3 = 2.5-6.2 years). Of the 80 patients, 21 (26.3%) patients had AF recurrence after ablation. There were no significant differences between AF recurrence vs. no recurrence groups in age, gender, CHA2DS2-VASc score, or baseline comorbidities. At baseline, patients with AF recurrence compared to without recurrence had lower LV end systolic volume index (32 ± 7 vs 37 ± 11 mL/m2; p = 0.045) and lower ℇCT (7.1 ± 4.6 vs 9.1 ± 3.7; p = 0.05). Post-ablation, patients with AF recurrence had higher LA minimum volume (68 ± 32 vs 55 ± 23; p = 0.05), right atrial volume index (62 ± 20 vs 52 ± 19 mL/m2; p = 0.04) and lower LA active ejection fraction (24 ± 8 vs 29 ± 11; p = 0.05), LA total ejection fraction (39 ± 14 vs 46 ± 12; p = 0.02), LA expansion index (73.6 ± 37.5 vs 94.7 ± 37.1; p = 0.03) and ℇCT (6.2 ± 2.9 vs 7.3 ± 1.7; p = 0.04). Adjusting for clinical variables in the multivariate logistic regression model, post-ablation minimum LA volume (OR 1.09; CI 1.02-1.16), LA expansion index (OR 0.98; CI 0.96-0.99), and baseline ℇR (OR 0.92; CI 0.85-0.99) were independently associated with AF recurrence.
Conclusion: Significant changes in LA volumes and strain parameters occur after AF ablation. CMR derived baseline ℇR, post-ablation minimum LAV, and expansion index are independently associated with AF recurrence.
Keywords: Atrial fibrillation; Cardiovascular magnetic resonance; Catheter ablation; Left atrial strain; Recurrence.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Atrial fibrillation: current understandings and research imperatives. The National Heart, Lung, and Blood Institute Working Group on Atrial Fibrillation. J Am Coll Cardiol 1993;22:1830–4. - PubMed
-
- Sievers B, Kirchberg S, Addo M, Bakan A, Brandts B, Trappe HJ. Assessment of left atrial volumes in sinus rhythm and atrial fibrillation using the biplane area-length method and cardiovascular magnetic resonance imaging with TrueFISP. J Cardiovasc Magn Reson. 2004;6:855–863. doi: 10.1081/JCMR-200036170. - DOI - PubMed
-
- Kuppahally SS, Akoum N, Burgon NS, et al. Left atrial strain and strain rate in patients with paroxysmal and persistent atrial fibrillation: relationship to left atrial structural remodeling detected by delayed-enhancement MRI. Circ Cardiovasc Imag. 2010;3:231–239. doi: 10.1161/CIRCIMAGING.109.865683. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
