

Ventricular flow analysis and its association with exertional capacity in repaired tetralogy of Fallot: 4D flow cardiovascular magnetic resonance study
- PMID: 34980199
- PMCID: PMC8722058
- DOI: 10.1186/s12968-021-00832-2
Ventricular flow analysis and its association with exertional capacity in repaired tetralogy of Fallot: 4D flow cardiovascular magnetic resonance study
Abstract
Background: Four-dimensional (4D) flow cardiovascular magnetic resonance (CMR) allows quantification of biventricular blood flow by flow components and kinetic energy (KE) analyses. However, it remains unclear whether 4D flow parameters can predict cardiopulmonary exercise testing (CPET) as a clinical outcome in repaired tetralogy of Fallot (rTOF). Current study aimed to (1) compare 4D flow CMR parameters in rTOF with age- and gender-matched healthy controls, (2) investigate associations of 4D flow parameters with functional and volumetric right ventricular (RV) remodelling markers, and CPET outcome.
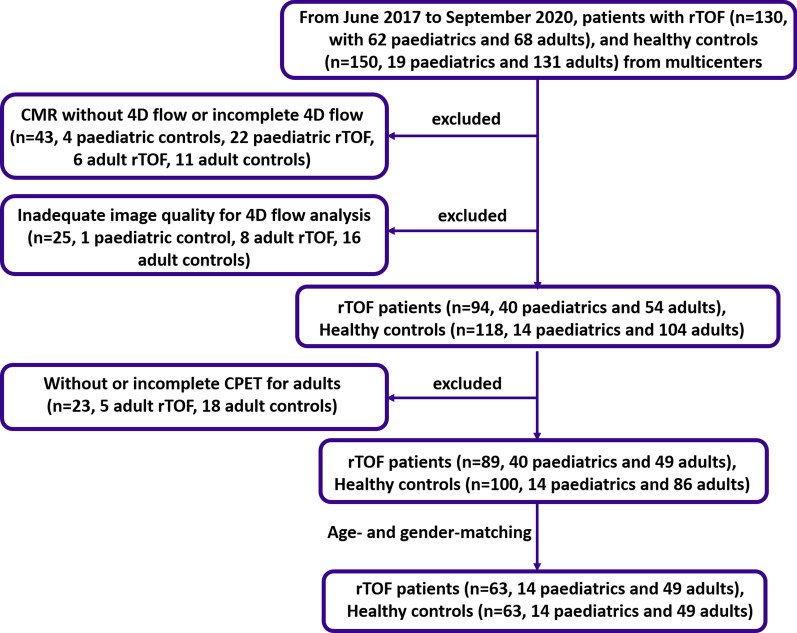
Methods: Sixty-three rTOF patients (14 paediatric, 49 adult; 30 ± 15 years; 29 M) and 63 age- and gender-matched healthy controls (14 paediatric, 49 adult; 31 ± 15 years) were prospectively recruited at four centers. All underwent cine and 4D flow CMR, and all adults performed standardized CPET same day or within one week of CMR. RV remodelling index was calculated as the ratio of RV to left ventricular (LV) end-diastolic volumes. Four flow components were analyzed: direct flow, retained inflow, delayed ejection flow and residual volume. Additionally, three phasic KE parameters normalized to end-diastolic volume (KEiEDV), were analyzed for both LV and RV: peak systolic, average systolic and peak E-wave.
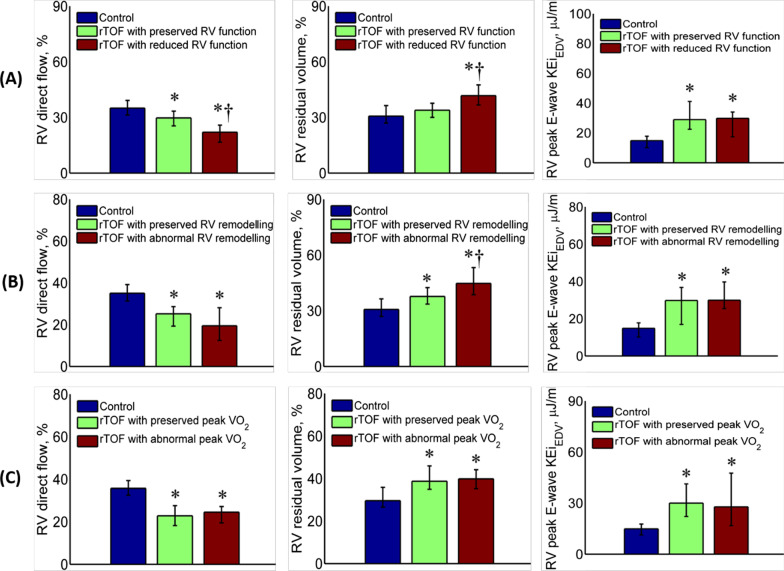
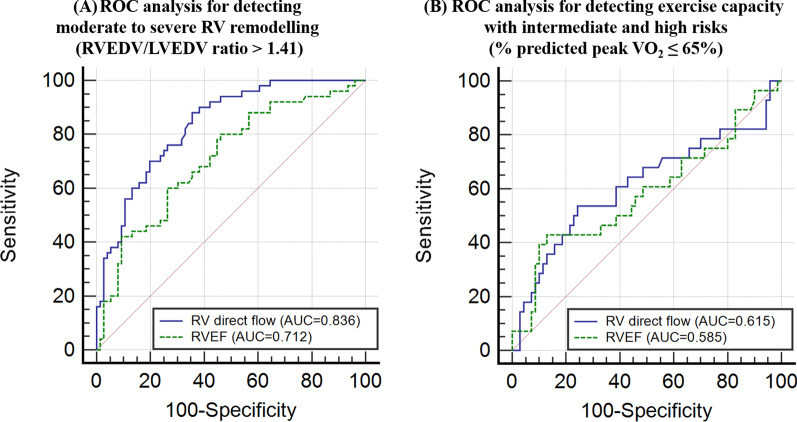
Results: In comparisons of rTOF vs. healthy controls, median LV retained inflow (18% vs. 16%, P = 0.005) and median peak E-wave KEiEDV (34.9 µJ/ml vs. 29.2 µJ/ml, P = 0.006) were higher in rTOF; median RV direct flow was lower in rTOF (25% vs. 35%, P < 0.001); median RV delayed ejection flow (21% vs. 17%, P < 0.001) and residual volume (39% vs. 31%, P < 0.001) were both greater in rTOF. RV KEiEDV parameters were all higher in rTOF than healthy controls (all P < 0.001). On multivariate analysis, RV direct flow was an independent predictor of RV function and CPET outcome. RV direct flow and RV peak E-wave KEiEDV were independent predictors of RV remodelling index.
Conclusions: In this multi-scanner multicenter 4D flow CMR study, reduced RV direct flow was independently associated with RV dysfunction, remodelling and, to a lesser extent, exercise intolerance in rTOF patients. This supports its utility as an imaging parameter for monitoring disease progression and therapeutic response in rTOF. Clinical Trial Registration https://www.clinicaltrials.gov . Unique identifier: NCT03217240.
Keywords: 4D flow CMR; Cardiopulmonary exercise testing; Flow components; Kinetic energy; Repaired tetralogy of Fallot.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Apitz C, Webb GD, Redington AN. Tetralogy of fallot. Lancet. 2009;374:1462–1471. - PubMed
-
- Valente AM, Geva T. How to Image Repaired Tetralogy of Fallot. Circ Cardiovasc Imaging. 2017;10:e004270. - PubMed
-
- Gatzoulis MA, Balaji S, Webber SA, Siu SC, Hokanson JS, Poile C, et al. Risk factors for arrhythmia and sudden cardiac death late after repair of tetralogy of Fallot: a multicentre study. Lancet. 2000;356:975–981. - PubMed
-
- Friedberg MK, Fernandes FP, Roche SL, Grosse-Wortmann L, Manlhiot C, Fackoury C, et al. Impaired right and left ventricular diastolic myocardial mechanics and filling in asymptomatic children and adolescents after repair of tetralogy of Fallot. Eur Heart J Cardiovasc Imaging. 2012;13:905–913. - PubMed
-
- Diller GP, Kempny A, Liodakis E, Alonso-Gonzalez R, Inuzuka R, Uebing A, et al. Left ventricular longitudinal function predicts life-threatening ventricular arrhythmia and death in adults with repaired tetralogy of fallot. Circulation. 2012;125:2440–2446. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
