

Mechanical power in pediatric acute respiratory distress syndrome: a PARDIE study
- PMID: 34980228
- PMCID: PMC8722295
- DOI: 10.1186/s13054-021-03853-6
Mechanical power in pediatric acute respiratory distress syndrome: a PARDIE study
Abstract
Background: Mechanical power is a composite variable for energy transmitted to the respiratory system over time that may better capture risk for ventilator-induced lung injury than individual ventilator management components. We sought to evaluate if mechanical ventilation management with a high mechanical power is associated with fewer ventilator-free days (VFD) in children with pediatric acute respiratory distress syndrome (PARDS).
Methods: Retrospective analysis of a prospective observational international cohort study.
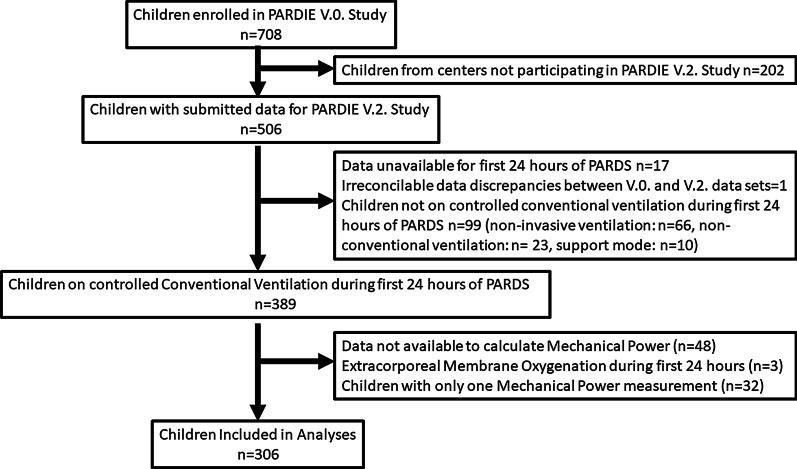
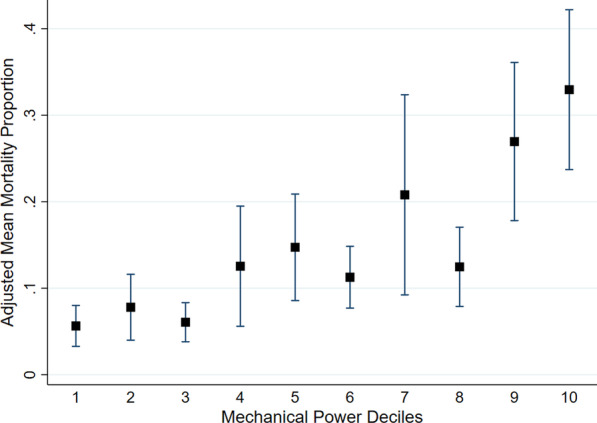
Results: There were 306 children from 55 pediatric intensive care units included. High mechanical power was associated with younger age, higher oxygenation index, a comorbid condition of bronchopulmonary dysplasia, higher tidal volume, higher delta pressure (peak inspiratory pressure-positive end-expiratory pressure), and higher respiratory rate. Higher mechanical power was associated with fewer 28-day VFD after controlling for confounding variables (per 0.1 J·min-1·Kg-1 Subdistribution Hazard Ratio (SHR) 0.93 (0.87, 0.98), p = 0.013). Higher mechanical power was not associated with higher intensive care unit mortality in multivariable analysis in the entire cohort (per 0.1 J·min-1·Kg-1 OR 1.12 [0.94, 1.32], p = 0.20). But was associated with higher mortality when excluding children who died due to neurologic reasons (per 0.1 J·min-1·Kg-1 OR 1.22 [1.01, 1.46], p = 0.036). In subgroup analyses by age, the association between higher mechanical power and fewer 28-day VFD remained only in children < 2-years-old (per 0.1 J·min-1·Kg-1 SHR 0.89 (0.82, 0.96), p = 0.005). Younger children were managed with lower tidal volume, higher delta pressure, higher respiratory rate, lower positive end-expiratory pressure, and higher PCO2 than older children. No individual ventilator management component mediated the effect of mechanical power on 28-day VFD.
Conclusions: Higher mechanical power is associated with fewer 28-day VFDs in children with PARDS. This association is strongest in children < 2-years-old in whom there are notable differences in mechanical ventilation management. While further validation is needed, these data highlight that ventilator management is associated with outcome in children with PARDS, and there may be subgroups of children with higher potential benefit from strategies to improve lung-protective ventilation.
Take home message: Higher mechanical power is associated with fewer 28-day ventilator-free days in children with pediatric acute respiratory distress syndrome. This association is strongest in children <2-years-old in whom there are notable differences in mechanical ventilation management.
Keywords: Critical care; Mechanical; Pediatrics; Ventilator-induced lung injury; Ventilators.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
