

Esmolol response in septic shock patients in relation to vascular waterfall phenomenon measured by critical closure pressure and mean systemic filling pressure: a prospective observational study
- PMID: 34980284
- PMCID: PMC8725571
- DOI: 10.1186/s40560-021-00587-z
Esmolol response in septic shock patients in relation to vascular waterfall phenomenon measured by critical closure pressure and mean systemic filling pressure: a prospective observational study
Abstract
Background: Bedside measurements of critical closure pressure (Pcc) and mean systemic circulation filling pressure (Pmsf) were utilized to evaluate the response to esmolol in septic shock patients, in relation to the vascular waterfall phenomenon and body oxygen supply and demand.
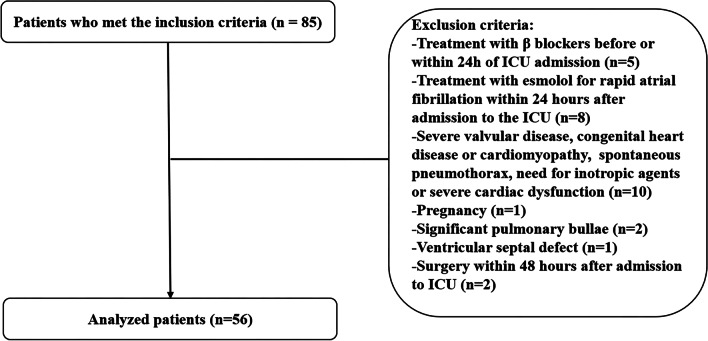
Methods: This prospective observational self-controlled study included patients with septic shock, newly admitted to the intensive care unit, between August 2019 and January 2021. Pcc and Pmsf, along with the heart rate and other hemodynamic indicators were observed and compared before and 1 h after esmolol IV infusion.
Results: After 24 h of initial hemodynamic optimization, 56 patients were finally enrolled. After start of esmolol infusion, patients had a significant decrease in cardiac index (CI) (4.0 vs. 3.3 L/min/m2, P < 0.001), a significant increase in stroke index (SI) (34.1 vs. 36.6 mL/m2, P < 0.01), and a significant decrease in heart rate (HR) (116.8 vs. 90.6 beats/min, P < 0.001). After 1 h of treatment with esmolol, patients had a significant increase in Pcc (31.4 vs. 36.7 mmHg, P < 0.01). The difference between Pcc and Pmsf before and after treatment was statistically different (4.0 vs. 10.0 mmHg, P < 0.01). After heart rate control with esmolol, the patients had a significant increase in the body circulation vascular resistance indices (RIs) (15.14 vs. 18.25 mmHg/min/m2/L, P < 0.001). There was an increase in ScvO2 in patients after treatment with esmolol, but the difference was not statistically significant (68.4% vs. 69.8%, P > 0.05), while Pcv-aCO2 was significantly lower (6.3 vs. 4.9 mmHg, P < 0.001) and patients had a significant decrease in blood lactate levels (4.0 vs. 3.6 mmol/L, P < 0.05).
Conclusion: Patients with septic shock whose heart rate is greater than 95 beats/min after hemodynamic optimization were treated with esmolol, which could effectively control heart rate and reduce CI, as well as improve Pcc and increase the difference between Pcc and Pmsf (known as "vascular waterfall" phenomenon), without affecting MAP, CVP, Pmsf and arteriovenous vascular resistance, and improve the balance of oxygen supply and demand in the body.
Keywords: Critical closure pressure; Esmolol; Mean systemic circulation filling pressure; Septic shock; Vascular waterfall.
© 2021. The Author(s).
Conflict of interest statement
None of the authors declare any conflicts of interest.
Figures



References
LinkOut - more resources
Full Text Sources
