

Evidence for Menopause as a Sex-Specific Risk Factor for Glaucoma
- PMID: 34981287
- PMCID: PMC9250947
- DOI: 10.1007/s10571-021-01179-z
Evidence for Menopause as a Sex-Specific Risk Factor for Glaucoma
Abstract
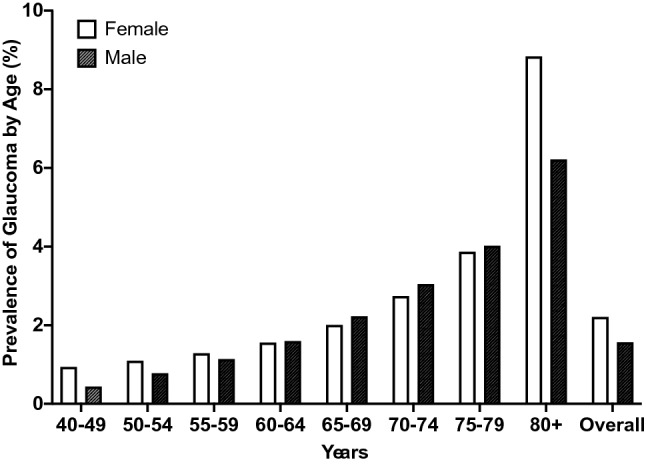
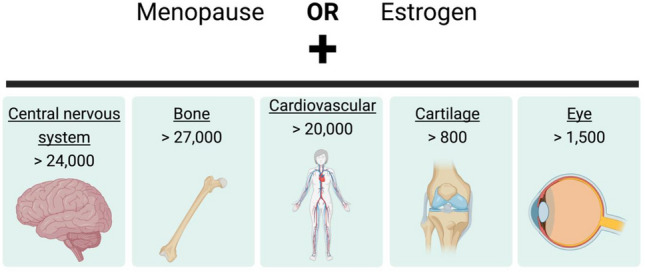
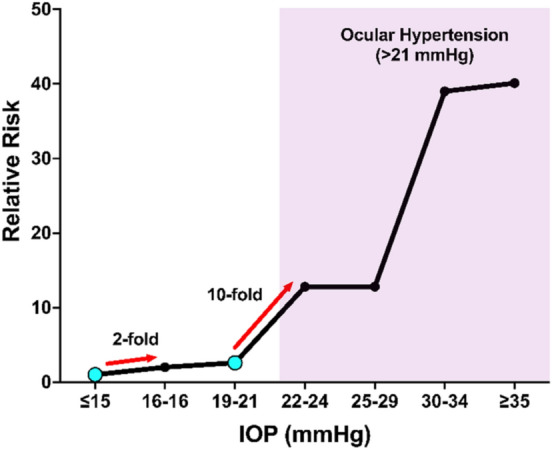
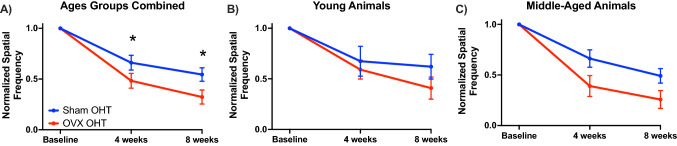
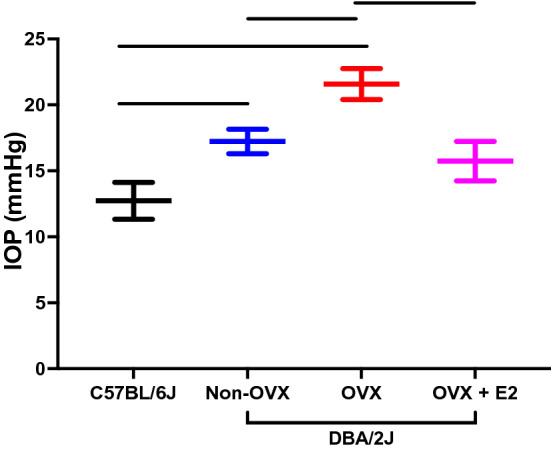
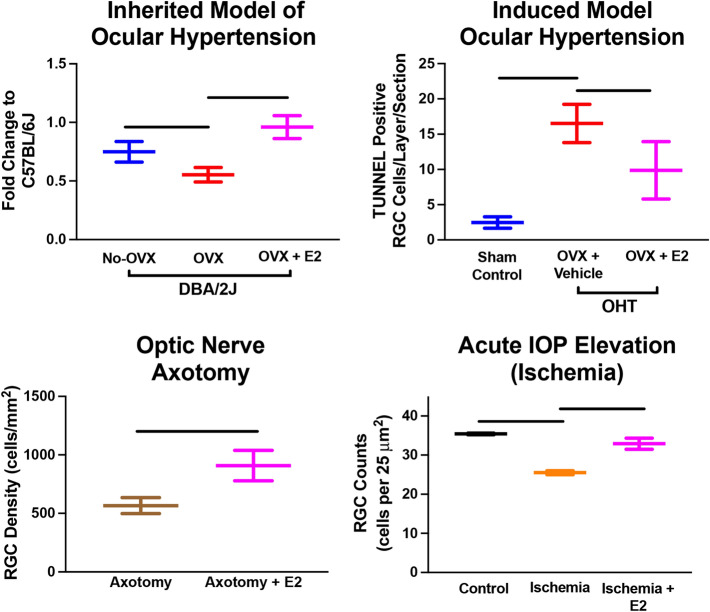
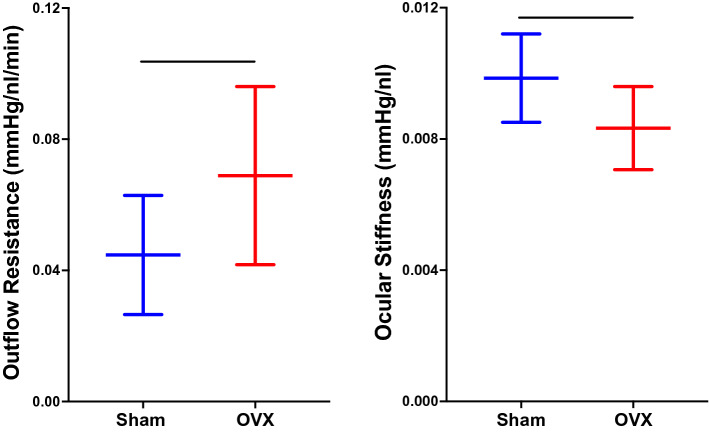
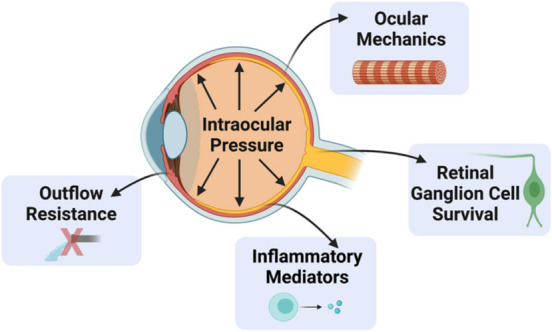
Glaucoma is a leading cause of irreversible blindness worldwide and is characterized by progressive loss of visual function and retinal ganglion cells (RGC). Current epidemiological, clinical, and basic science evidence suggest that estrogen plays a role in the aging of the optic nerve. Menopause, a major biological life event affecting all women, coincides with a decrease in circulating sex hormones, such as estrogen. While 59% of the glaucomatous population are females, sex is not considered a risk factor for developing glaucoma. In this review, we explore whether menopause is a sex-specific risk factor for glaucoma. First, we investigate how menopause is defined as a sex-specific risk factor for other pathologies, including cardiovascular disease, osteoarthritis, and bone health. Next, we discuss clinical evidence that highlights the potential role of menopause in glaucoma. We also highlight preclinical studies that demonstrate larger vision and RGC loss following surgical menopause and how estrogen is protective in models of RGC injury. Lastly, we explore how surgical menopause and estrogen signaling are related to risk factors associated with developing glaucoma (e.g., intraocular pressure, aqueous outflow resistance, and ocular biomechanics). We hypothesize that menopause potentially sets the stage to develop glaucoma and therefore is a sex-specific risk factor for this disease.
Keywords: Biomechanics; Estrogen; Glaucoma; Intraocular pressure; Menopause; Outflow resistance; Ovariectomy; Retinal ganglion cells; Sex specific; Visual function.
© 2021. This is a U.S. government work and not under copyright protection in the U.S.; foreign copyright protection may apply.
Figures

References
-
- ACOG Committee Opinion No. 651: Menstruation in girls and adolescents: using the menstrual cycle as a vital sign. Obstet Gynecol 126:e143–e146. 10.1097/AOG.0000000000001215 - PubMed
-
- Affinito P et al (2003) Effects of hormone replacement therapy on ocular function in postmenopause. Menopause 10:482–487. 10.1097/01.GME.0000063568.84134.35 - PubMed
-
- Agency, C. I. (ed Langley (VA): CIA) (World Factbook [Internet]) (2010)
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
