

Dual-energy CT: minimal essentials for radiologists
- PMID: 34981319
- PMCID: PMC9162973
- DOI: 10.1007/s11604-021-01233-2
Dual-energy CT: minimal essentials for radiologists
Abstract
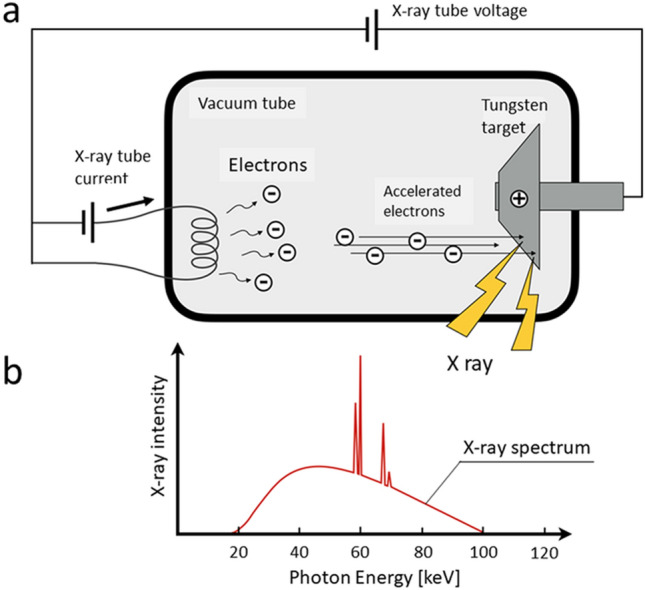
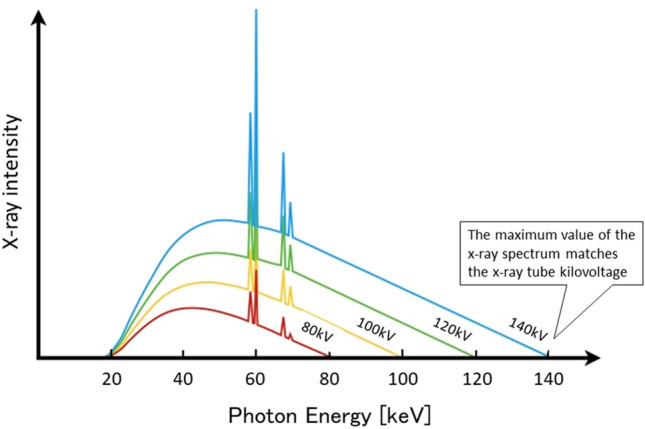
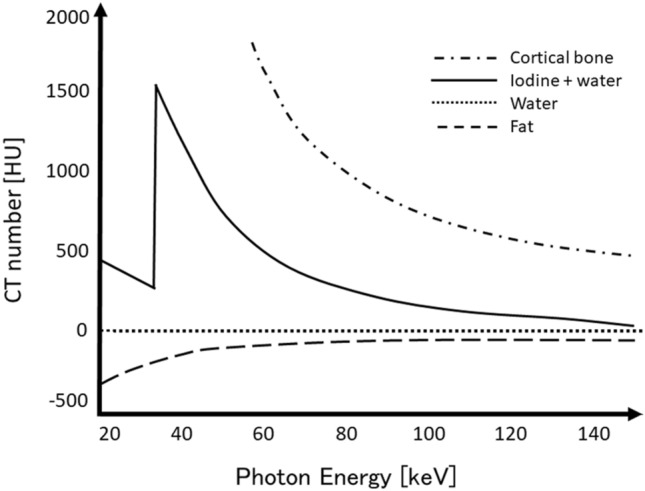
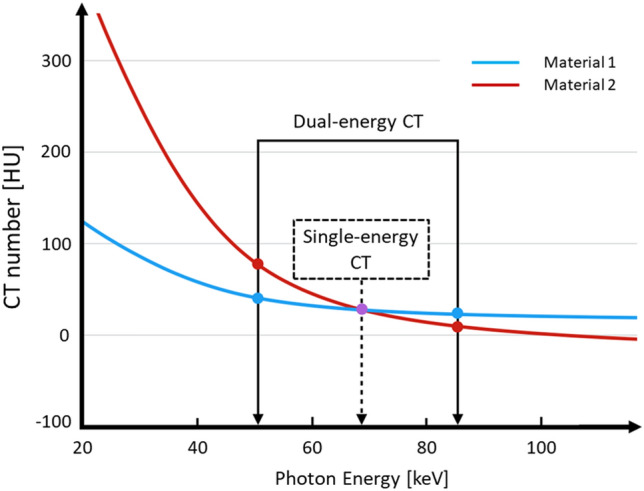
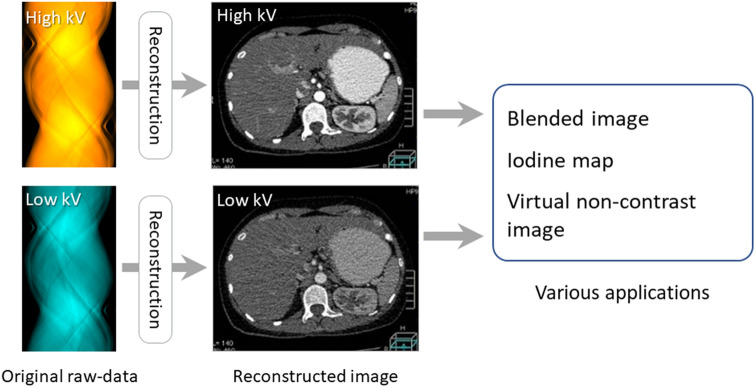
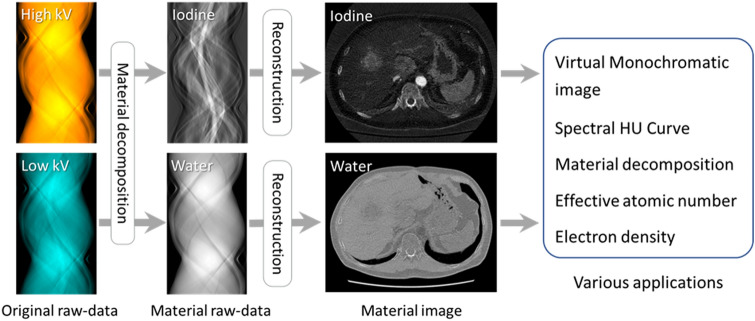
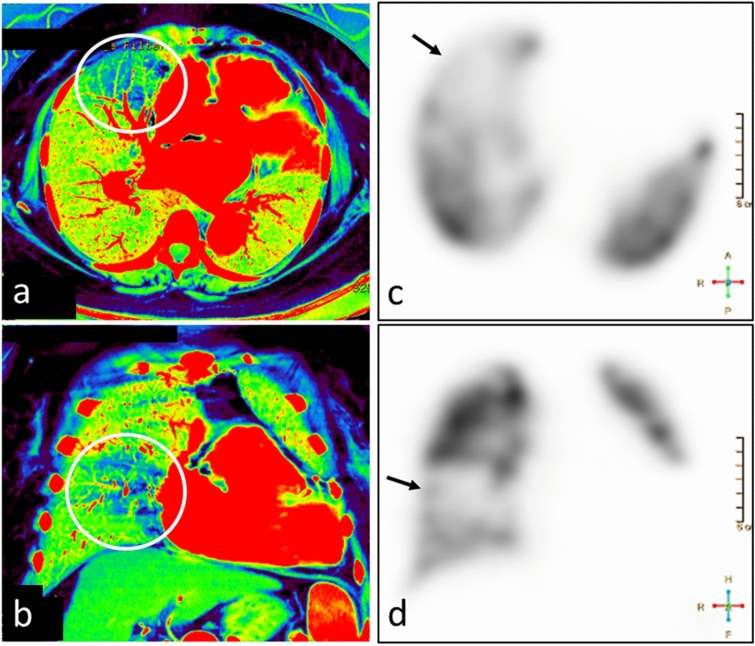
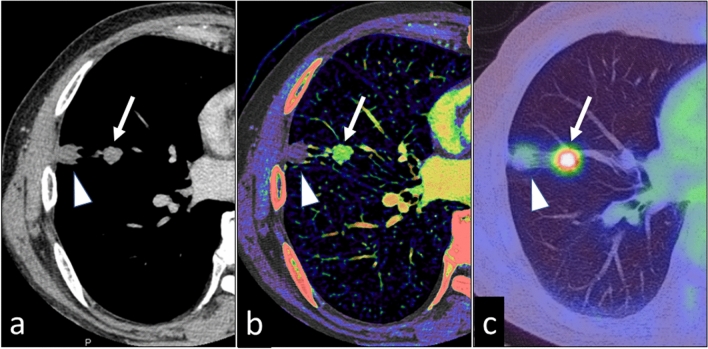
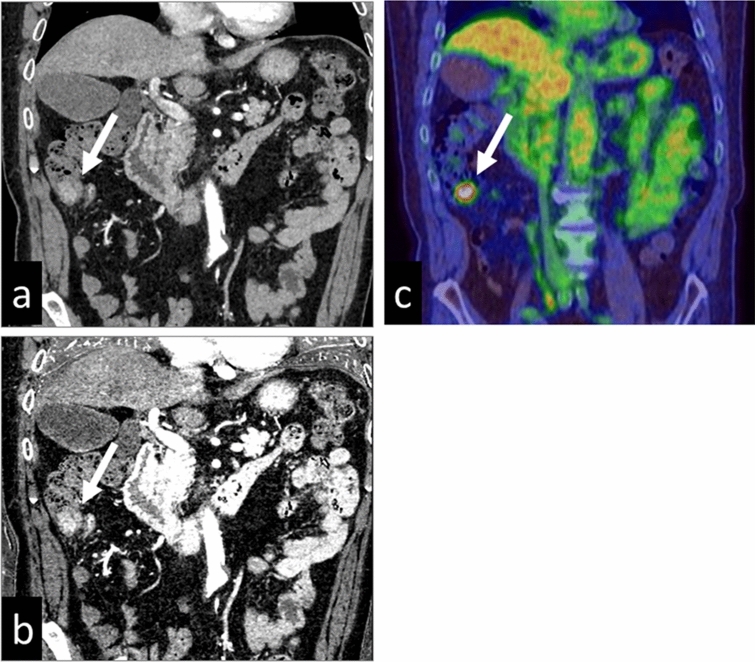
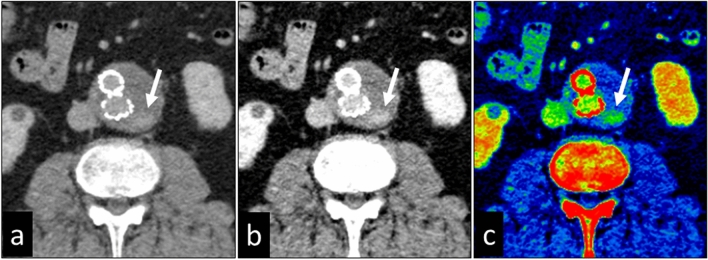
Dual-energy CT, the object is scanned at two different energies, makes it possible to identify the characteristics of materials that cannot be evaluated on conventional single-energy CT images. This imaging method can be used to perform material decomposition based on differences in the material-attenuation coefficients at different energies. Dual-energy analyses can be classified as image data-based- and raw data-based analysis. The beam-hardening effect is lower with raw data-based analysis, resulting in more accurate dual-energy analysis. On virtual monochromatic images, the iodine contrast increases as the energy level decreases; this improves visualization of contrast-enhanced lesions. Also, the application of material decomposition, such as iodine- and edema images, increases the detectability of lesions due to diseases encountered in daily clinical practice. In this review, the minimal essentials of dual-energy CT scanning are presented and its usefulness in daily clinical practice is discussed.
Keywords: Computed tomography; Detectability; Dual-energy CT; Material decomposition.
© 2021. The Author(s).
Conflict of interest statement
K.A. is currently receiving a research grant from Canon Medical Systems Corp. For the remaining authors none were declared.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
