

Reliability, Validity, and Responsiveness of the DEG, a Three-Item Dyspnea Measure
- PMID: 34981344
- PMCID: PMC9360273
- DOI: 10.1007/s11606-021-07307-1
Reliability, Validity, and Responsiveness of the DEG, a Three-Item Dyspnea Measure
Abstract
Background: Dyspnea is a common and debilitating symptom that affects many different patient populations. Dyspnea measures should assess multiple domains.
Objective: To evaluate the reliability, validity, and responsiveness of an ultra-brief, multi-dimensional dyspnea measure.
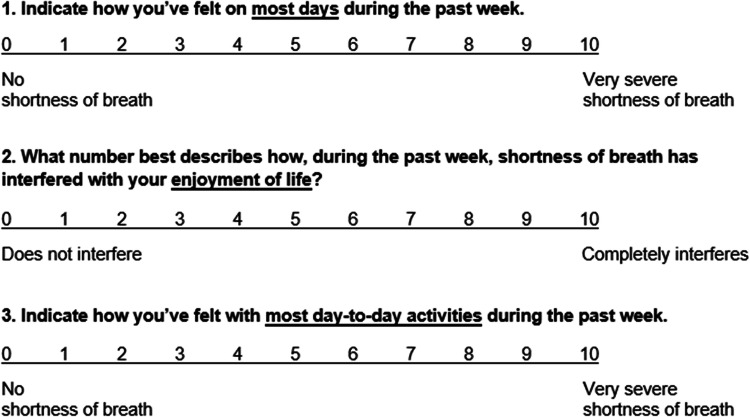
Design: We adapted the DEG from the PEG, a valid 3-item pain measure, to assess average dyspnea intensity (D), interference with enjoyment of life (E), and dyspnea burden with general activity (G).
Participants: We used data from a multi-site randomized clinical trial among outpatients with heart failure.
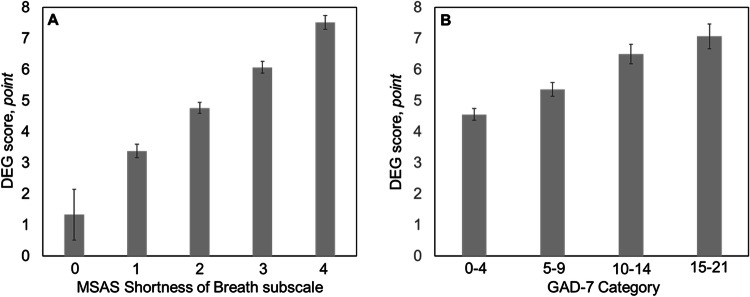
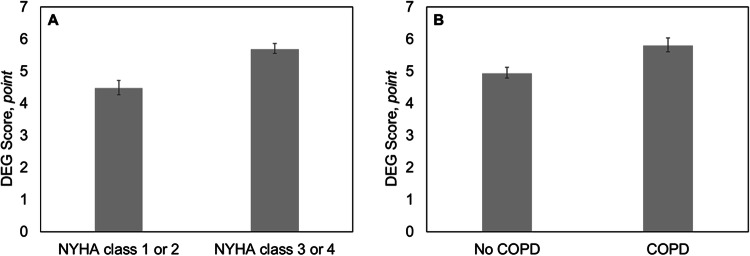
Main measures: We evaluated reliability (Cronbach's alpha), concurrent validity with the Memorial-Symptom-Assessment-Scale (MSAS) shortness-of-breath distress-orbothersome item and 7-item Generalized-Anxiety-Disorder (GAD-7) scale, knowngroups validity with New-York-Heart-Association-Functional-Classification (NYHA) 1-2 or 3-4 and presence or absence of comorbid chronic obstructive pulmonary disease (COPD), responsiveness with the MSAS item as an anchor, and calculated a minimal clinically important difference (MCID) using distribution methods.
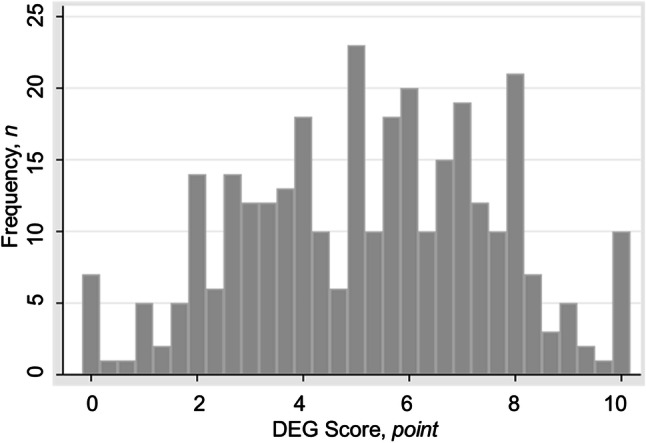
Key results: Among 312 participants, the DEG was reliable (Cronbach's alpha 0.92). The mean (standard deviation) DEG score was 5.26 (2.36) (range 0-10) points. DEG scores correlated strongly with the MSAS shortness of breath distress-or-bothersome item (r=0.66) and moderately with GAD-7 categories (ρ=0.36). DEG scores were statistically significantly lower among patients with NYHA 1-2 compared to 3-4 [mean difference (standard error): 1.22 (0.27) points, p<0.01], and those without compared to with comorbid COPD [0.87 (0.27) points, p<0.01]. The DEG was highly sensitive to change, with MCID of 0.59-1.34 points, or 11-25% change.
Conclusions: The novel, ultra-brief DEG measure is reliable, valid, and highly responsive. Future studies should evaluate the DEG's sensitivity to interventions, use anchor-based methods to triangulate MCID estimates, and determine its prognostic usefulness among patients with chronic cardiopulmonary and other diseases.
Keywords: Patient-reported outcome measure; cardiopulmonary disease; chronic obstructive pulmonary disease; dyspnea; heart failure; psychometrics.
© 2021. This is a U.S. government work and not under copyright protection in the U.S.; foreign copyright protection may apply.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
A meta-analysis of four randomized clinical trials to confirm the reliability and responsiveness of the Shortness of Breath with Daily Activities (SOBDA) questionnaire in chronic obstructive pulmonary disease.Health Qual Life Outcomes. 2015 Oct 31;13:177. doi: 10.1186/s12955-015-0369-3. Health Qual Life Outcomes. 2015. PMID: 26520062 Free PMC article.
-
Item selection, reliability and validity of the Shortness of Breath with Daily Activities (SOBDA) questionnaire: a new outcome measure for evaluating dyspnea in chronic obstructive pulmonary disease.Health Qual Life Outcomes. 2013 Nov 14;11:196. doi: 10.1186/1477-7525-11-196. Health Qual Life Outcomes. 2013. PMID: 24229361 Free PMC article.
-
Validity, reliability, and responsiveness of a new short Visual Simplified Respiratory Questionnaire (VSRQ) for health-related quality of life assessment in chronic obstructive pulmonary disease.Int J Chron Obstruct Pulmon Dis. 2009;4:9-18. Epub 2009 Apr 15. Int J Chron Obstruct Pulmon Dis. 2009. PMID: 19436682 Free PMC article.
-
Minimally clinically important difference for the UCSD Shortness of Breath Questionnaire, Borg Scale, and Visual Analog Scale.COPD. 2005 Mar;2(1):105-10. doi: 10.1081/copd-200050655. COPD. 2005. PMID: 17136970 Review.
-
The MCID of the transition dyspnea index is a total score of one unit.COPD. 2005 Mar;2(1):99-103. doi: 10.1081/copd-200050666. COPD. 2005. PMID: 17136969 Review.
Cited by
-
Comparative responsiveness and minimally important difference of Fatigue Symptom Inventory (FSI) scales and the FSI-3 in trials with cancer survivors.J Patient Rep Outcomes. 2022 Jul 23;6(1):82. doi: 10.1186/s41687-022-00488-1. J Patient Rep Outcomes. 2022. PMID: 35870034 Free PMC article.
-
How Does Spiritual Well-Being Change Over Time Among US Patients with Heart Failure and What Predicts Change?J Relig Health. 2024 Aug;63(4):3050-3065. doi: 10.1007/s10943-022-01712-4. Epub 2022 Dec 7. J Relig Health. 2024. PMID: 36478542
References
-
- Hendriks SA, Smalbrugge M, Galindo-Garre F, Hertogh CM, van der Steen JT. From admission to death: prevalence and course of pain, agitation, and shortness of breath, and treatment of these symptoms in nursing home residents with dementia. J Am Med Dir Assoc. 2015;16(6):475–481. doi: 10.1016/j.jamda.2014.12.016. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
