

Frailty and Survival After In-Hospital Cardiopulmonary Resuscitation
- PMID: 34981346
- PMCID: PMC9585129
- DOI: 10.1007/s11606-021-07199-1
Frailty and Survival After In-Hospital Cardiopulmonary Resuscitation
Abstract
Background: Older adults face high mortality following resuscitation efforts for in-hospital cardiac arrest. Less is known about the role of frailty in survival to discharge after in-hospital cardiopulmonary resuscitation.
Objective: To investigate whether frailty, measured by the Clinical Frailty Scale, is associated with mortality after cardiopulmonary resuscitation following in-hospital cardiac arrest in older adults in the USA.
Design: Retrospective cohort study.
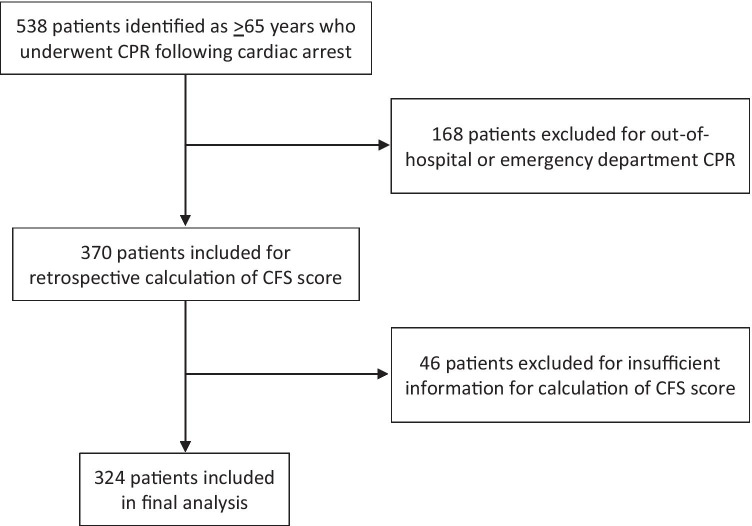
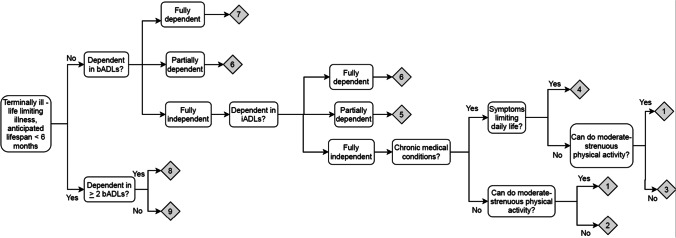
Participants: Patients ≥ 65 years who had undergone cardiopulmonary resuscitation during an inpatient admission at two urban academic hospitals and three suburban community hospitals within a Boston area healthcare system from January 2018-January 2020. Patients with Clinical Frailty Scale scores 1-3 were considered not frail, 4-6 were considered very mildly, mildly, and moderately frail, respectively, and 7-9 were considered severely frail.
Main measures: In-hospital mortality after cardiopulmonary resuscitation.
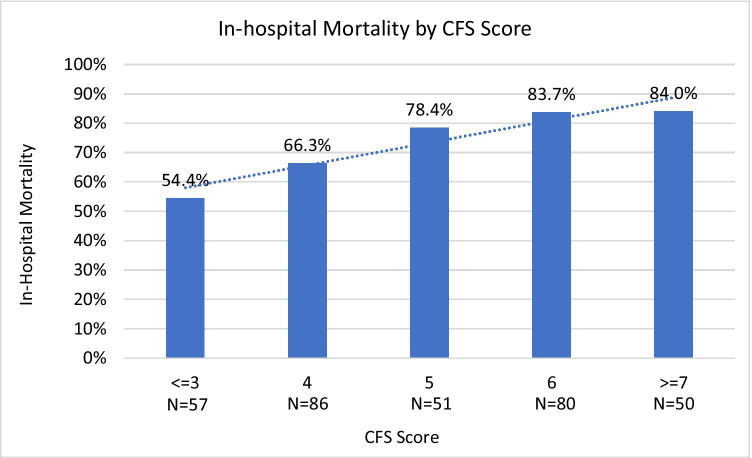
Key results: Among 324 patients who underwent cardiopulmonary resuscitation following in-hospital cardiac arrest, 73.1% experienced in-hospital mortality. Patients with a Clinical Frailty Scale score of 1-3 had 54% in-hospital mortality, which increased to 66%, 78%, 84%, and 84% for those with a Clinical Frailty Scale score of 4, 5, 6, and 7-9, respectively (p = 0.001). After adjusting for age, sex, race, and Charlson Comorbidity Index, higher frailty scores were significantly associated with higher odds of in-hospital mortality. Compared to those with a Clinical Frailty Scale score of 1-3, odds ratios (95% CI) for in-hospital mortality for patients with a Clinical Frailty Scale score of 4, 5, 6, and 7-9 were 1.6 (0.8-3.3), 3.0 (1.3-7.1), 4.4 (1.9-9.9), and 4.6 (1.8-11.8), respectively (p = 0.001).
Conclusions: Higher levels of frailty are associated with increased mortality after in-hospital cardiopulmonary resuscitation in older adults. Clinicians may consider using the Clinical Frailty Scale to help guide goals of care conversations, including discussion of code status, in this patient population.
Keywords: cardiopulmonary resuscitation; frailty; geriatrics; goals of care.
© 2021. Society of General Internal Medicine.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
