

Implementation of an Intensive Telehealth Intervention for Rural Patients with Clinic-Refractory Diabetes
- PMID: 34981358
- PMCID: PMC8722663
- DOI: 10.1007/s11606-021-07281-8
Implementation of an Intensive Telehealth Intervention for Rural Patients with Clinic-Refractory Diabetes
Abstract
Background: Rural patients with type 2 diabetes (T2D) may experience poor glycemic control due to limited access to T2D specialty care and self-management support. Telehealth can facilitate delivery of comprehensive T2D care to rural patients, but implementation in clinical practice is challenging.
Objective: To examine the implementation of Advanced Comprehensive Diabetes Care (ACDC), an evidence-based, comprehensive telehealth intervention for clinic-refractory, uncontrolled T2D. ACDC leverages existing Veterans Health Administration (VHA) Home Telehealth (HT) infrastructure, making delivery practical in rural areas.
Design: Mixed-methods implementation study.
Participants: 230 patients with clinic-refractory, uncontrolled T2D.
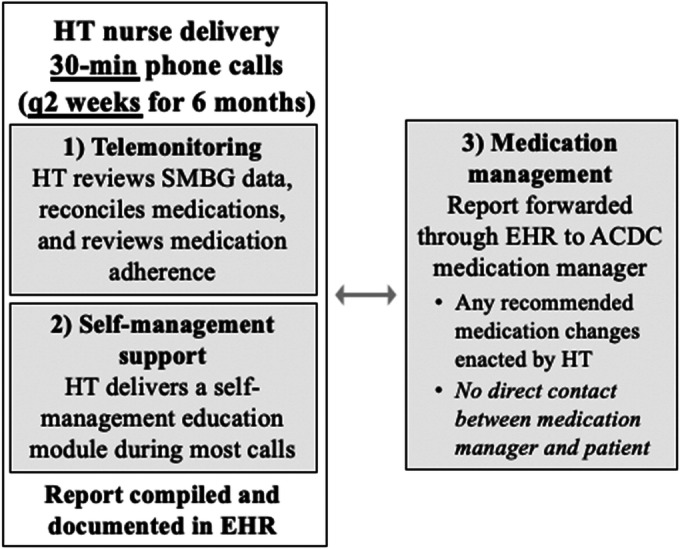
Intervention: ACDC bundles telemonitoring, self-management support, and specialist-guided medication management, and is delivered over 6 months using existing VHA HT clinical staffing/equipment. Patients may continue in a maintenance protocol after the initial 6-month intervention period.
Main measures: Implementation was evaluated using the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework. The primary effectiveness outcome was hemoglobin A1c (HbA1c).
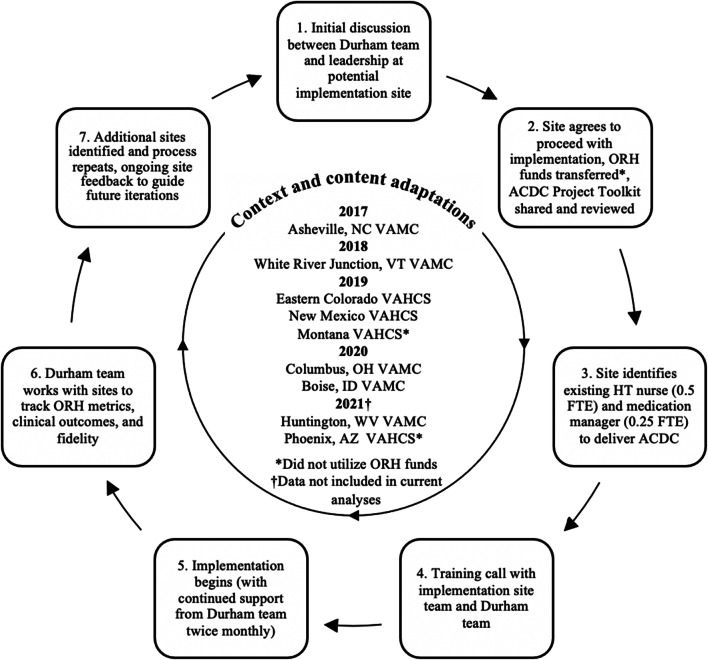
Key results: From 2017 to 2020, ACDC was delivered to 230 patients across seven geographically diverse VHA sites; on average, patients were 59 years of age, 95% male, 80% white, and 14% Hispanic/Latinx. Patients completed an average of 10.1 of 12 scheduled encounters during the 6-month intervention period. Model-estimated mean baseline HbA1c was 9.56% and improved to 8.14% at 6 months (- 1.43%, 95% CI: - 1.64, - 1.21; P < .001). Benefits persisted at 12 (- 1.26%, 95% CI: - 1.48, - 1.05; P < .001) and 18 months (- 1.08%, 95% CI - 1.35, - 0.81; P < .001). Patients reported increased engagement in self-management and awareness of glycemic control, while clinicians and HT nurses reported a moderate workload increase. As of this submission, some sites have maintained delivery of ACDC for up to 4 years.
Conclusions: When strategically designed to leverage existing infrastructure, comprehensive telehealth interventions can be implemented successfully, even in rural areas. ACDC produced sustained improvements in glycemic control in a previously refractory population.
Keywords: diabetes mellitus, type 2; health services research; implementation science; rural health; telemedicine.
© 2021. This is a U.S. government work and not under copyright protection in the U.S.; foreign copyright protection may apply.
Conflict of interest statement
Dr. Bosworth reports research grants from the PhRMA Foundation, Proteus Digital Health, Otsuka, Novo Nordisk, Sanofi, Improved Patient Outcomes, Boehinger Ingelheim, NIH, and VA as well as consulting from Sanofi, Novartis, Otsuka, Abbott, Xcenda, Preventric Diagnostics, Boehringer Ingelheim, and the Medicines Company. None of this work relates to the current study. Dr. Lewinski reports receiving funds from PhRMA Foundation and Otsuka; none of this work relates to the current study. The remaining authors have no competing interests to declare.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
