

Prediction of Upstaging in Ductal Carcinoma in Situ Based on Mammographic Radiomic Features
- PMID: 34981975
- PMCID: PMC8962778
- DOI: 10.1148/radiol.210407
Prediction of Upstaging in Ductal Carcinoma in Situ Based on Mammographic Radiomic Features
Abstract
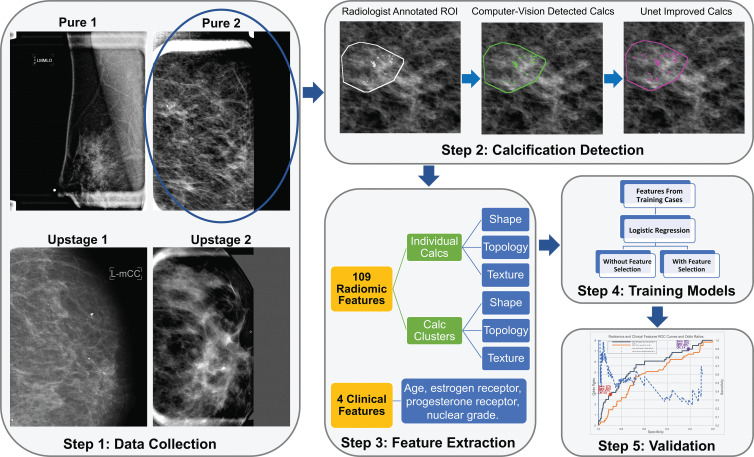
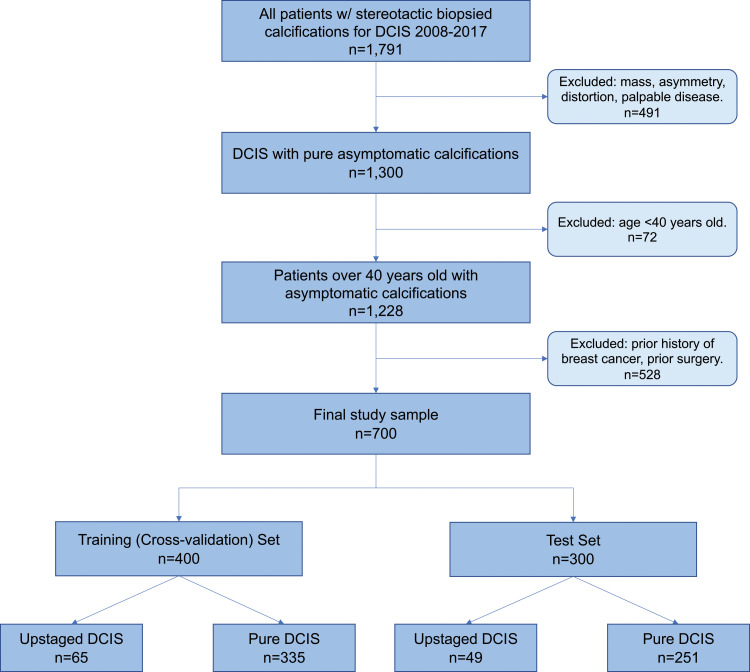
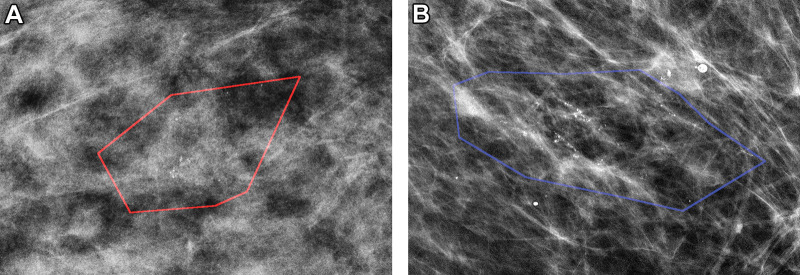
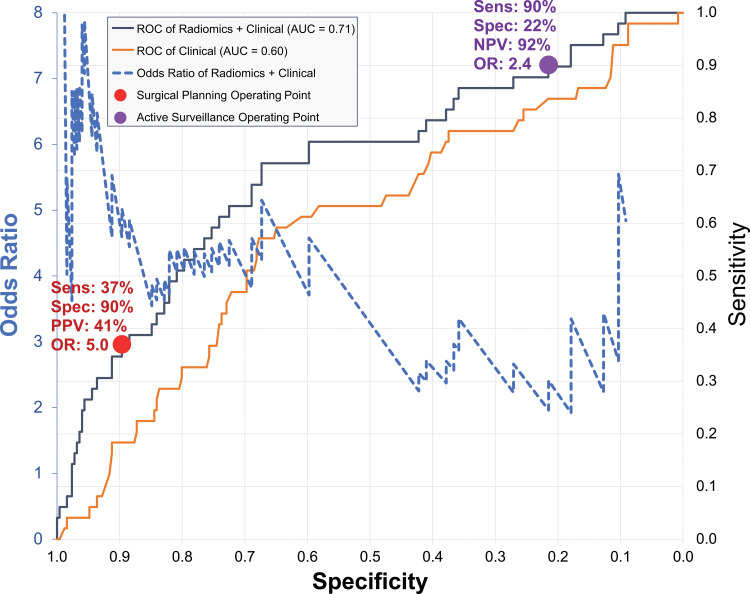
Background Improving diagnosis of ductal carcinoma in situ (DCIS) before surgery is important in choosing optimal patient management strategies. However, patients may harbor occult invasive disease not detected until definitive surgery. Purpose To assess the performance and clinical utility of mammographic radiomic features in the prediction of occult invasive cancer among women diagnosed with DCIS on the basis of core biopsy findings. Materials and Methods In this Health Insurance Portability and Accountability Act-compliant retrospective study, digital magnification mammographic images were collected from women who underwent breast core-needle biopsy for calcifications that was performed at a single institution between September 2008 and April 2017 and yielded a diagnosis of DCIS. The database query was directed at asymptomatic women with calcifications without a mass, architectural distortion, asymmetric density, or palpable disease. Logistic regression with regularization was used. Differences across training and internal test set by upstaging rate, age, lesion size, and estrogen and progesterone receptor status were assessed by using the Kruskal-Wallis or χ2 test. Results The study consisted of 700 women with DCIS (age range, 40-89 years; mean age, 59 years ± 10 [standard deviation]), including 114 with lesions (16.3%) upstaged to invasive cancer at subsequent surgery. The sample was split randomly into 400 women for the training set and 300 for the testing set (mean ages: training set, 59 years ± 10; test set, 59 years ± 10; P = .85). A total of 109 radiomic and four clinical features were extracted. The best model on the test set by using all radiomic and clinical features helped predict upstaging with an area under the receiver operating characteristic curve of 0.71 (95% CI: 0.62, 0.79). For a fixed high sensitivity (90%), the model yielded a specificity of 22%, a negative predictive value of 92%, and an odds ratio of 2.4 (95% CI: 1.8, 3.2). High specificity (90%) corresponded to a sensitivity of 37%, positive predictive value of 41%, and odds ratio of 5.0 (95% CI: 2.8, 9.0). Conclusion Machine learning models that use radiomic features applied to mammographic calcifications may help predict upstaging of ductal carcinoma in situ, which can refine clinical decision making and treatment planning. © RSNA, 2022.
Conflict of interest statement
Figures
References
-
- Siegel RL , Miller KD , Jemal A . Cancer statistics, 2020 . CA Cancer J Clin 2020. ; 70 ( 1 ): 7 – 30 . - PubMed
-
- Sanders ME , Schuyler PA , Dupont WD , Page DL . The natural history of low-grade ductal carcinoma in situ of the breast in women treated by biopsy only revealed over 30 years of long-term follow-up . Cancer 2005. ; 103 ( 12 ): 2481 – 2484 . - PubMed
-
- Hieken TJ , Krishnamurthy V , Farolan M , Velasco JM . Long-term outcome of DCIS patients: p53 as a biomarker of ipsilateral recurrence . J Clin Oncol 2011. ; 29 ( 27_suppl ): 39 .
-
- Schulz S , Sinn P , Golatta M , et al. . Prediction of underestimated invasiveness in patients with ductal carcinoma in situ of the breast on percutaneous biopsy as rationale for recommending concurrent sentinel lymph node biopsy . Breast 2013. ; 22 ( 4 ): 537 – 542 . - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
