

Assessment of Hypothetical Out-of-Pocket Costs of Guideline-Recommended Medications for the Treatment of Older Adults With Multiple Chronic Conditions, 2009 and 2019
- PMID: 34982097
- PMCID: PMC8728660
- DOI: 10.1001/jamainternmed.2021.7457
Assessment of Hypothetical Out-of-Pocket Costs of Guideline-Recommended Medications for the Treatment of Older Adults With Multiple Chronic Conditions, 2009 and 2019
Abstract
Importance: Most adults 65 years or older have multiple chronic conditions. Managing these conditions with prescription drugs can be costly, particularly for older adults with limited incomes.
Objective: To estimate hypothetical out-of-pocket costs associated with guideline-recommended outpatient medications for the initial treatment of 8 common chronic diseases among older adults with Medicare prescription drug plans (PDPs).
Design, setting, and participants: This retrospective cross-sectional study used 2009 and 2019 Medicare prescription drug plan formulary files to estimate annual out-of-pocket costs among hypothetical patients enrolled in Medicare Advantage or stand-alone Medicare Part D plans. A total of 3599 PDPs in 2009 and 3618 PDPs in 2019 were included after inclusion and exclusion criteria were applied. Costs associated with guideline-recommended medications for 8 of the most common chronic diseases (atrial fibrillation, chronic obstructive pulmonary disease [COPD], heart failure with reduced ejection fraction, hypercholesterolemia, hypertension, osteoarthritis, osteoporosis, and type 2 diabetes), alone and in 2 clusters of commonly comorbid conditions, were examined.
Main outcomes and measures: Annual out-of-pocket costs for each chronic condition, inflation adjusted to 2019 dollars.
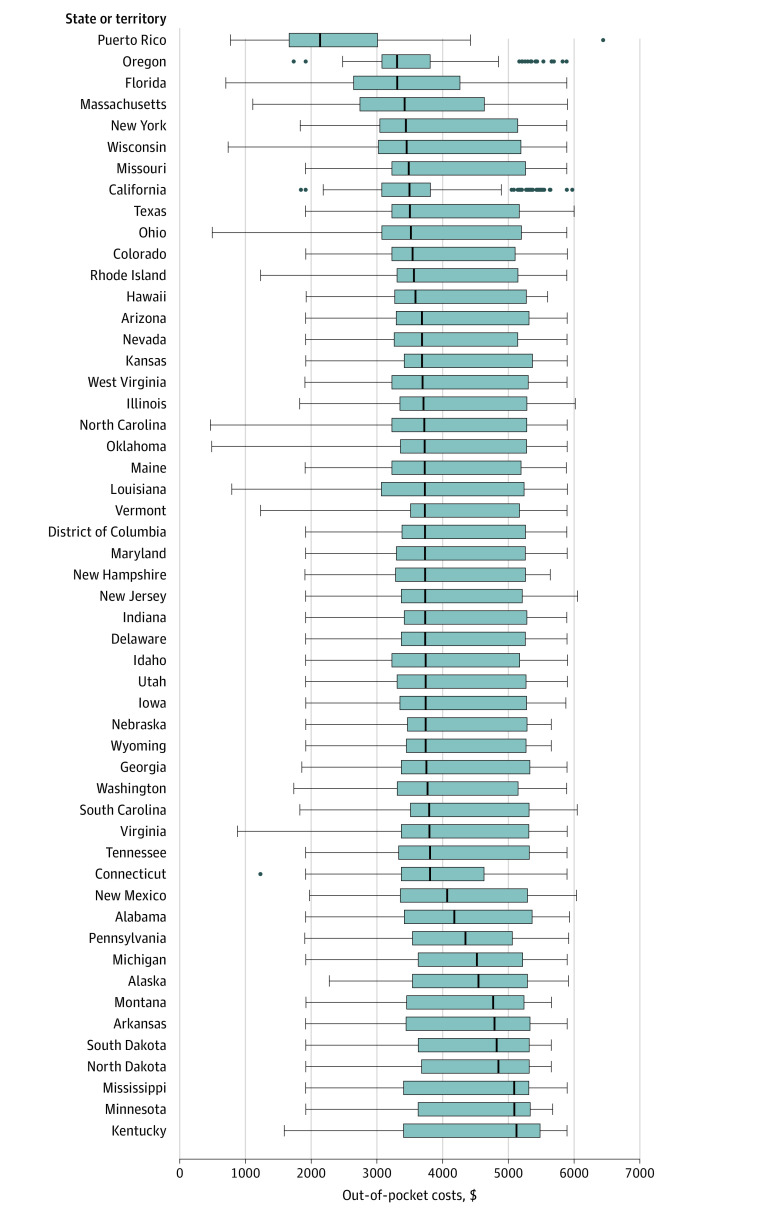
Results: Among 3599 Medicare PDPs in 2009, 1998 were Medicare Advantage plans and 1601 were stand-alone plans; among 3618 Medicare PDPs in 2019, 2719 were Medicare Advantage plans and 899 were stand-alone plans. For an older adult enrolled in any Medicare PDP in 2019, the median annual out-of-pocket costs for individual conditions varied, from a minimum of $32 (IQR, $6-$48) for guideline-recommended management of osteoporosis (a decrease from $128 [IQR, $102-$183] in 2009) to a maximum of $1579 (IQR, $1524-$2229) for guideline-recommended management of atrial fibrillation (an increase from $91 [IQR, $73-$124] in 2009). For an older adult with a cluster of 5 commonly comorbid conditions (COPD, hypertension, osteoarthritis, osteoporosis, and type 2 diabetes) enrolled in any PDP, the median out-of-pocket cost in 2019 was $1999 (IQR, $1630-$2564), a 12% decrease from $2284 (IQR, $1920-$3107) in 2009. For an older adult with all 8 chronic conditions (atrial fibrillation, COPD, diabetes, hypercholesterolemia, heart failure, hypertension, osteoarthritis, and osteoporosis) enrolled in any PDP, the median out-of-pocket cost in 2019 was $3630 (IQR, $3234-$5197), a 41% increase from $2571 (IQR, $2185-$3719) in 2009.
Conclusions and relevance: In this cross-sectional study, out-of-pocket costs for guideline-recommended outpatient medications for the initial treatment of 8 common chronic diseases varied by condition. Although costs generally decreased between 2009 and 2019, particularly with regard to conditions for which generic drugs were available, out-of-pocket costs remained high and may have presented a substantial financial burden for Medicare beneficiaries, especially older adults with conditions for which brand-name drugs were guideline recommended.
Conflict of interest statement
Figures

Comment in
-
Persistent Prescription Drug Affordability Challenges for Medicare Beneficiaries With Multiple Chronic Conditions-What Goes Up Must Come Down?JAMA Intern Med. 2022 Feb 1;182(2):195-196. doi: 10.1001/jamainternmed.2021.7454. JAMA Intern Med. 2022. PMID: 34982096 No abstract available.
References
-
- Centers for Medicare & Medicaid Services . Chronic conditions among Medicare beneficiaries: chartbook: 2017 edition. Accessed August 20, 2020. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Tren...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
