Presence and predominance of histological grade 3 define cT1HG bladder cancer prognostic groups
- PMID: 34983119
- PMCID: PMC8756148
- DOI: 10.4111/icu.20210386
Presence and predominance of histological grade 3 define cT1HG bladder cancer prognostic groups
Abstract
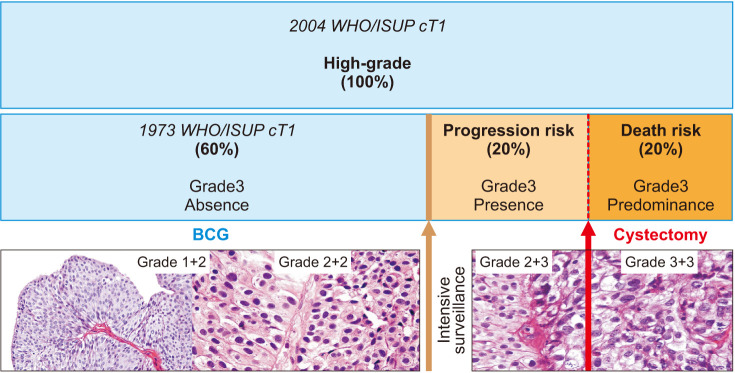
Purpose: Current World Health Organization/International Society of Urological Pathology (2004 WHO/ISUP) grading of bladder urothelial carcinoma relies on the highest pathologic grade of the specimen and does not reflect the inherent qualitative and quantitative heterogeneity of disease.
Materials and methods: We retrospectively studied consecutive urothelial high-grade cT1 (cT1HG) carcinomas submitted to adjuvant bacille Calmette-Guérin between 2008 and 2015 to evaluate the prognostic potential of grade 3 (presence or predominance) according to the 1973 WHO system concerning disease progression and cancer-specific death.
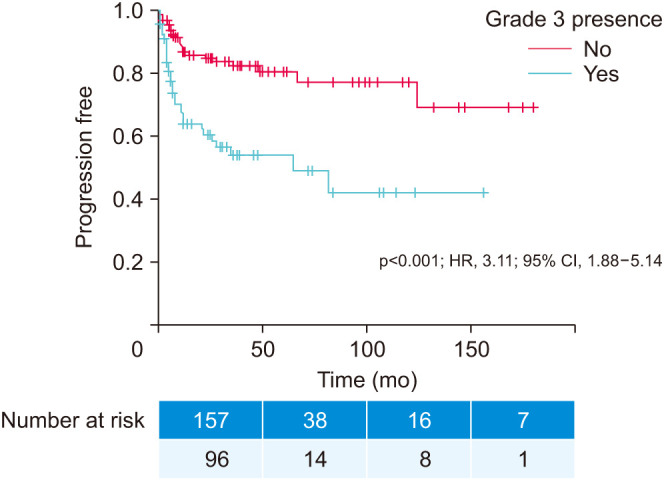
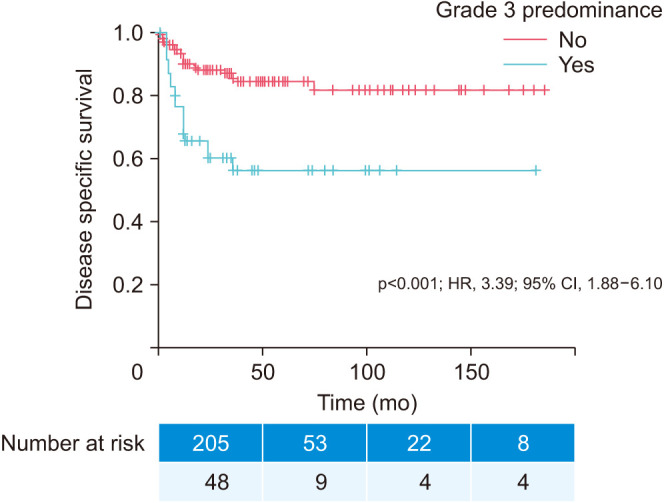
Results: Among 253 patients, grading distribution was 34.4% 1+2, 7.5% 2+1, 20.2% 2+2, 19.0% 2+3, 5.1% 3+2, and 13.8% 3+3. Recurrence was diagnosed in 115 (45.5%), progression in 83 (32.8%), and cancer-specific death in 50 patients (19.8%). Mean time to recurrence, progression, and death from disease were 35.9±31.7, 47.6±44.5, and 51.2±50.4 months, respectively. Grade 3 presence (2+3, 3+2, or 3+3) occurred in 96 (37.9%) and independently predicted time to progression (p<0.001; hazard ratio [HR], 3.11; 95% confidence interval [CI], 1.88-5.14). Grade 3 predominance (3+2 or 3+3) occurred in 48 (18.9%) and independently predicted time to disease-specific death.
Conclusions: Grade 3 presence and predominance are independent predictors of progression and disease-specific death and occur in about 40% and 20% of cT1HG, respectively. Describing qualitative and quantitative heterogeneity in urothelial carcinoma grading might improve the stratification of patients. This gives three prognostic high-grade groups based on WHO/ISUP 1973: prognostic grade group I (grade 3 absence), prognostic grade group II (grade 3 presence), and prognostic grade group III (grade 3 predominance).
Keywords: Histology; Prognosis; Urinary bladder neoplasms.
© The Korean Urological Association, 2022.
Conflict of interest statement
The authors have nothing to disclose.
Figures
Similar articles
-
Cancer heterogeneity and its biologic implications in the grading of urothelial carcinoma.Cancer. 2000 Apr 1;88(7):1663-70. doi: 10.1002/(sici)1097-0142(20000401)88:7<1663::aid-cncr21>3.0.co;2-8. Cancer. 2000. PMID: 10738225
-
International Society of Urological Pathology (ISUP) Consensus Conference on Current Issues in Bladder Cancer. Working Group 2: Grading of Mixed Grade, Invasive Urothelial Carcinoma Including Histologic Subtypes and Divergent Differentiations, and Non-Urothelial Carcinomas.Am J Surg Pathol. 2024 Jan 1;48(1):e11-e23. doi: 10.1097/PAS.0000000000002077. Epub 2023 Jun 29. Am J Surg Pathol. 2024. PMID: 37382156
-
Histological grading of papillary urothelial carcinoma of the bladder: prognostic value of the 1998 WHO/ISUP classification system and comparison with conventional grading systems.J Clin Pathol. 2002 Dec;55(12):900-5. doi: 10.1136/jcp.55.12.900. J Clin Pathol. 2002. PMID: 12461053 Free PMC article.
-
Head-to-head: how many categories for grading urothelial carcinoma?Histopathology. 2024 Feb;84(3):421-428. doi: 10.1111/his.15091. Epub 2023 Nov 7. Histopathology. 2024. PMID: 37936516 Review.
-
Urothelial neoplasms of the urinary bladder occurring in young adult and pediatric patients: a comprehensive review of literature with implications for patient management.Adv Anat Pathol. 2011 Jan;18(1):79-89. doi: 10.1097/PAP.0b013e318204c0cf. Adv Anat Pathol. 2011. PMID: 21169741 Review.
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin. 2021;71:7–33. - PubMed
-
- Schwaibold HE, Sivalingam S, May F, Hartung R. The value of a second transurethral resection for T1 bladder cancer. BJU Int. 2006;97:1199–1201. - PubMed
-
- Andrade DL, Moretti TBC, Neto WA, Benedetti J, Reis LO. Smoke load prognostic impact on bacillus Calmette-Guérin (BCG) treated non-muscle invasive bladder cancer. Int Urol Nephrol. 2020;52:1471–1476. - PubMed
-
- Bryan RT, Zeegers MP, James ND, Wallace DM, Cheng KK. Biomarkers in bladder cancer. BJU Int. 2010;105:608–613. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical