

Investigating the cognitive capacity constraints of an ICU care team using a systems engineering approach
- PMID: 34983402
- PMCID: PMC8724599
- DOI: 10.1186/s12871-021-01548-7
Investigating the cognitive capacity constraints of an ICU care team using a systems engineering approach
Abstract
Background: ICU operational conditions may contribute to cognitive overload and negatively impact on clinical decision making. We aimed to develop a quantitative model to investigate the association between the operational conditions and the quantity of medication orders as a measurable indicator of the multidisciplinary care team's cognitive capacity.
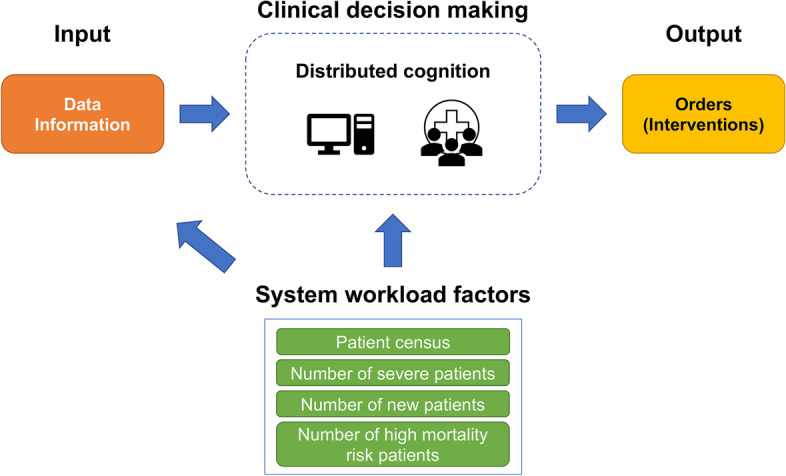
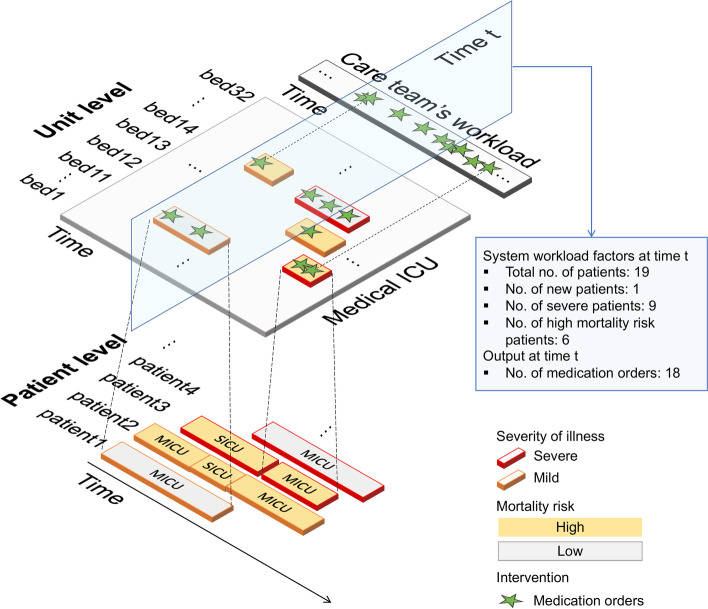
Methods: The temporal data of patients at one medical ICU (MICU) of Mayo Clinic in Rochester, MN between February 2016 to March 2018 was used. This dataset includes a total of 4822 unique patients admitted to the MICU and a total of 6240 MICU admissions. Guided by the Systems Engineering Initiative for Patient Safety model, quantifiable measures attainable from electronic medical records were identified and a conceptual framework of distributed cognition in ICU was developed. Univariate piecewise Poisson regression models were built to investigate the relationship between system-level workload indicators, including patient census and patient characteristics (severity of illness, new admission, and mortality risk) and the quantity of medication orders, as the output of the care team's decision making.
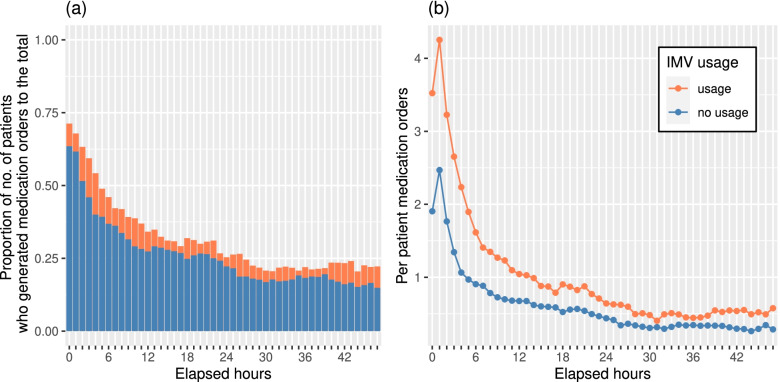
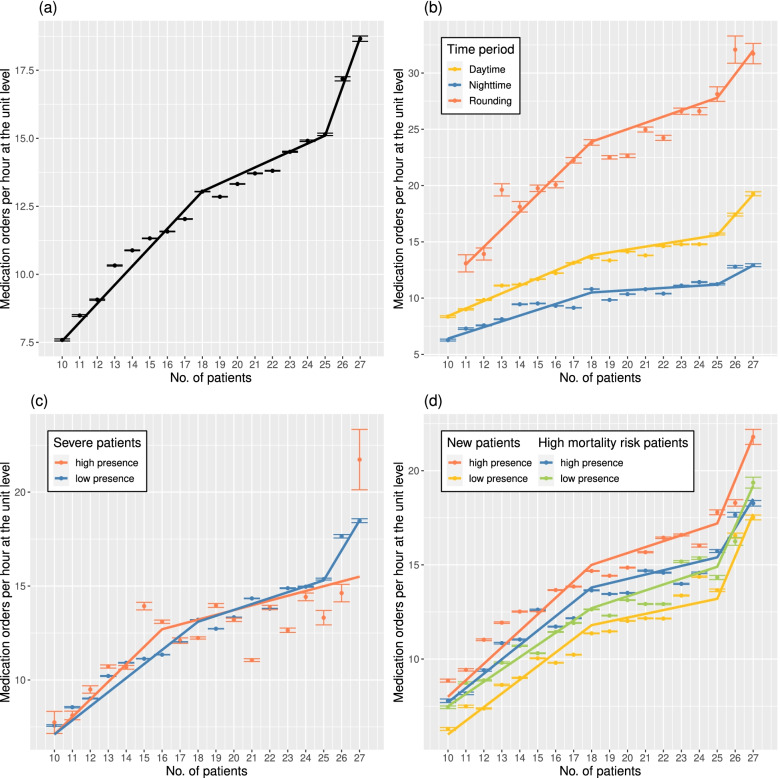
Results: Comparing the coefficients of different line segments obtained from the regression models using a generalized F-test, we identified that, when the ICU was more than 50% occupied (patient census > 18), the number of medication orders per patient per hour was significantly reduced (average = 0.74; standard deviation (SD) = 0.56 vs. average = 0.65; SD = 0.48; p < 0.001). The reduction was more pronounced (average = 0.81; SD = 0.59 vs. average = 0.63; SD = 0.47; p < 0.001), and the breakpoint shifted to a lower patient census (16 patients) when at a higher presence of severely-ill patients requiring invasive mechanical ventilation during their stay, which might be encountered in an ICU treating patients with COVID-19.
Conclusions: Our model suggests that ICU operational factors, such as admission rates and patient severity of illness may impact the critical care team's cognitive function and result in changes in the production of medication orders. The results of this analysis heighten the importance of increasing situational awareness of the care team to detect and react to changing circumstances in the ICU that may contribute to cognitive overload.
Keywords: Cognitive function; Electronic medical records; Organizational decision making; Situational awareness; Systems approach; Workload.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Harry E, Pierce RG, Kneeland P, Huang G, Stein J, Sweller J. Cognitive load and its implications for health care. NEJM Catalyst Published online March 14, 2018. https://catalyst.nejm.org/doi/full/10.1056/CAT.18.0233 - DOI
-
- Zhang Y, Padman R, Levin JE. Reducing Provider Cognitive Workload in CPOE Use: Optimizing Order Sets. MEDINFO 2013. Published online 2013:734–738. doi:10.3233/978-1-61499-289-9-734. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
