

Influence of coracoglenoid space on scapular neck fracture stability: biomechanical study
- PMID: 34983487
- PMCID: PMC8728935
- DOI: 10.1186/s12891-021-04974-3
Influence of coracoglenoid space on scapular neck fracture stability: biomechanical study
Abstract
Background: The anatomical variation of the coracoglenoid space has the potential to influence the stability of scapular neck fractures. This paper aimed to investigate the mechanical mechanism underlying the influence of different coracoglenoid space types on scapular neck fractures by morphometric analysis and biomechanical experiments.
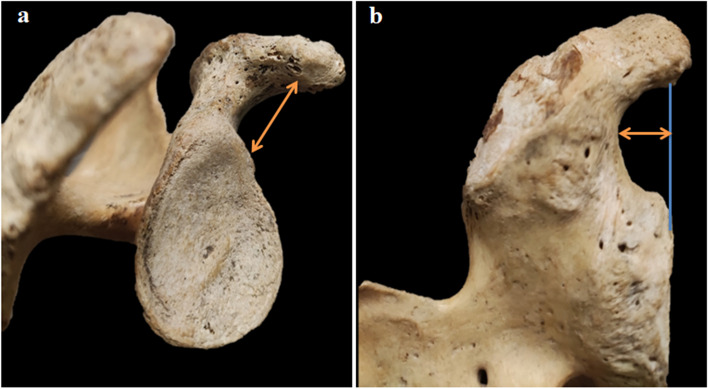
Methods: The morphology of 68 dried scapulae (left: 36; right: 32) was studied. Two variables, the length of the coracoglenoid distance (CGD) and the coracoglenoid notch (CGN), were measured. The distribution of CGN/CGD × 100% was used to identify the morphology of the coracoglenoid space. Each specimen was tested for failure under static axial compression loading. The average failure load, stiffness, and energy were calculated.
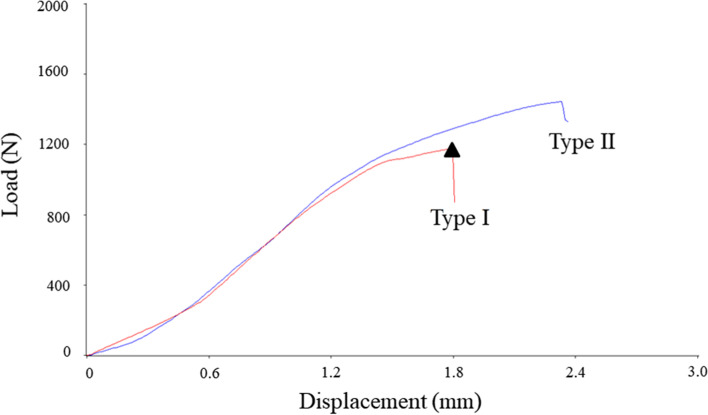
Results: Two coracoglenoid space types were identified. The incidence of Type I (''hook'' shape) was 53%, and that of Type II (''square bracket'' shape) was 47%. The CGD and CGN were significantly higher for type I than type II (13.81 ± 0.74 mm vs. 11.50 ± 1.03 mm, P < 0.05; 4.74 ± 0.45 mm vs. 2.61 ± 0.45 mm, P < 0.05). The average maximum failure load of the two types was 1270.82 ± 318.85 N and 1529.18 ± 467.29 N, respectively (P = 0.011). The stiffness and energy were significantly higher for type II than type I (896.75 ± 281.14 N/mm vs. 692.91 ± 217.95 N/mm, P = 0.001; 2100.38 ± 649.54 N × mm vs. 1712.71 ± 626.02 N × mm, P = 0.015).
Conclusions: There was great interindividual variation in the anatomical morphology of the coracoglenoid space. Type I (hook-like) spaces bore lower forces, were less stiff, and bore less energy, which may constitute an anatomical predisposition to scapular neck fractures.
Keywords: Biomechanics; Coracoglenoid space; Fractures; Scapular neck.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures






Similar articles
-
The coracoglenoid notch: anatomy and clinical significance.Surg Radiol Anat. 2021 Jan;43(1):11-17. doi: 10.1007/s00276-020-02527-2. Epub 2020 Jul 21. Surg Radiol Anat. 2021. PMID: 32696246
-
Mechanical testing of scapular neck fracture fixation using a synthetic bone model.Clin Biomech (Bristol). 2019 Jan;61:64-69. doi: 10.1016/j.clinbiomech.2018.11.007. Epub 2018 Nov 22. Clin Biomech (Bristol). 2019. PMID: 30496907
-
Comparing internal fixation constructs for scapular spine insufficiency fractures following reverse shoulder arthroplasty.J Shoulder Elbow Surg. 2021 Jan;30(1):172-177. doi: 10.1016/j.jse.2020.04.051. Epub 2020 Jun 9. J Shoulder Elbow Surg. 2021. PMID: 32788041 Clinical Trial.
-
Fractures of the anatomical neck of the scapula: two cases and review of the literature.Arch Orthop Trauma Surg. 2013 Aug;133(8):1115-9. doi: 10.1007/s00402-013-1783-9. Epub 2013 May 28. Arch Orthop Trauma Surg. 2013. PMID: 23712711 Review.
-
Headless Compression Screw Versus Kirschner Wire Fixation for Metacarpal Neck Fractures: A Biomechanical Study.J Hand Surg Am. 2017 May;42(5):392.e1-392.e6. doi: 10.1016/j.jhsa.2017.02.013. Epub 2017 Mar 27. J Hand Surg Am. 2017. PMID: 28359640
Cited by
-
Treatment options and outcomes for delayed scapular anatomical neck fractures: a case report and review of the literature.J Med Case Rep. 2024 Mar 9;18(1):94. doi: 10.1186/s13256-024-04424-3. J Med Case Rep. 2024. PMID: 38459542 Free PMC article. Review.
-
Finite element analysis of a novel anatomical locking plate for scapular neck fracture.J Orthop Surg Res. 2023 Mar 31;18(1):262. doi: 10.1186/s13018-023-03743-3. J Orthop Surg Res. 2023. PMID: 37004037 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
