

Telerehabilitation of acute musculoskeletal multi-disorders: prospective, single-arm, interventional study
- PMID: 34983488
- PMCID: PMC8728982
- DOI: 10.1186/s12891-021-04891-5
Telerehabilitation of acute musculoskeletal multi-disorders: prospective, single-arm, interventional study
Abstract
Background: Acute musculoskeletal (MSK) pain is very common and associated with impaired productivity and high economic burden. Access to timely and personalized, evidence-based care is key to improve outcomes while reducing healthcare expenditure. Digital interventions can facilitate access and ensure care scalability.
Objective: Present the feasibility and results of a fully remote digital care program (DCP) for acute MSK conditions affecting several body areas.
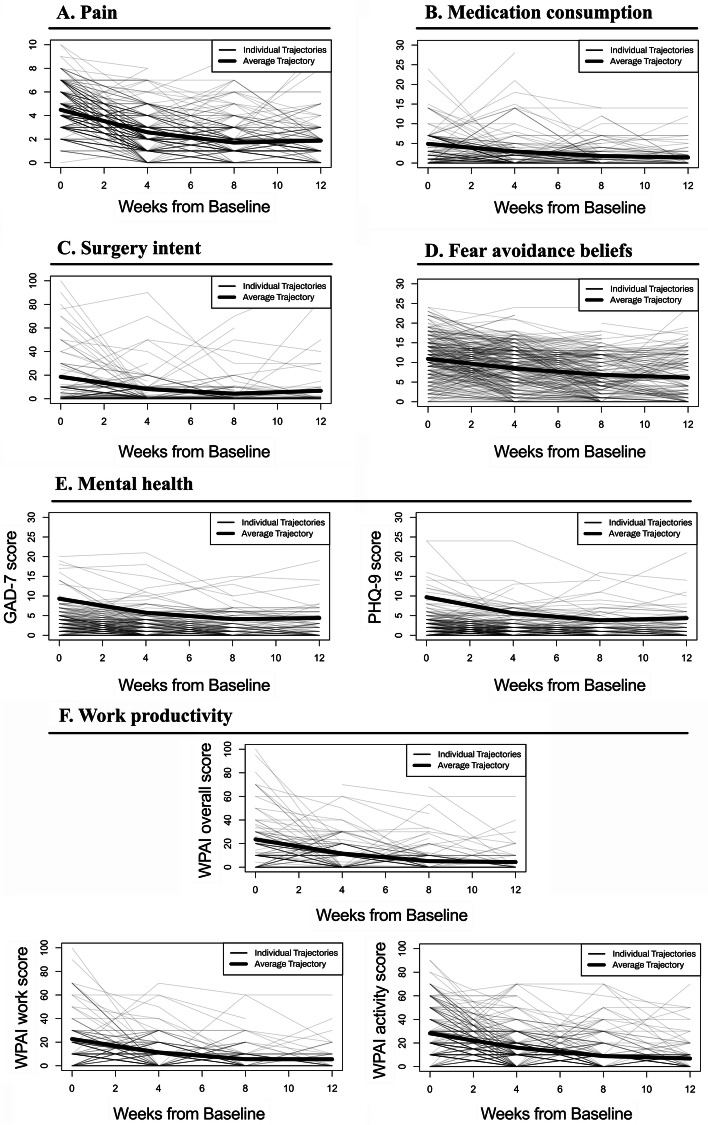
Methods: Interventional single-arm study of individuals applying for digital care programs for acute MSK pain. Primary outcome was the mean change between baseline and end-of-program in self-reported Numerical Pain Rating Scale (NPRS) score and secondary outcomes were change in analgesic consumption, intention to undergo surgery, anxiety (GAD-7), depression (PHQ-9), fear-avoidance beliefs (FABQ-PA), work productivity (WPAI-GH) and engagement.
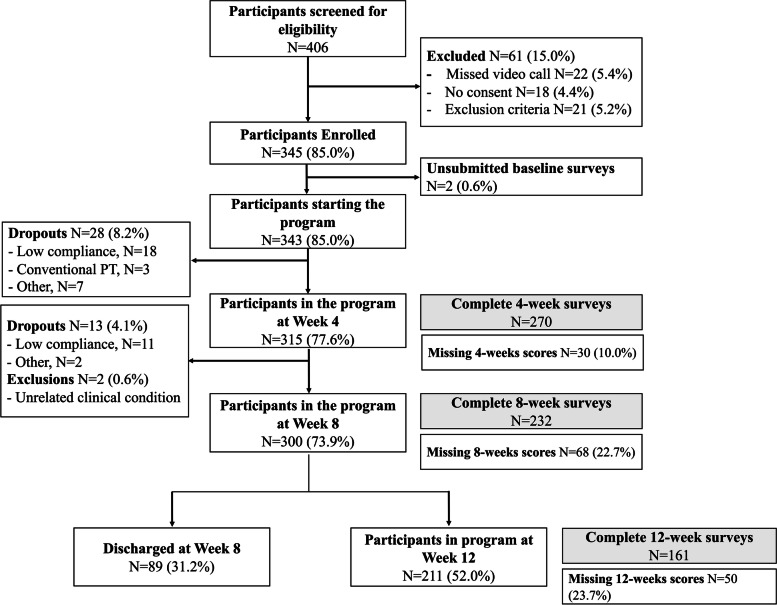
Results: Three hundred forty-three patients started the program, of which 300 (87.5%) completed the program. Latent growth curve analysis (LGCA) revealed that changes in NPRS between baseline and end-of-program were both statistically (p < 0.001) and clinically significant: 64.3% reduction (mean - 2.9 points). Marked improvements were also noted in all secondary outcomes: 82% reduction in medication intake, 63% reduction in surgery intent, 40% in fear-avoidance beliefs, 54% in anxiety, 58% in depression and 79% recovery in overall productivity. All outcomes had steeper improvements in the first 4 weeks, which paralleled higher engagement in this period (3.6 vs 3.2 overall weekly sessions, p < 0.001). Mean patient satisfaction score was 8.7/10 (SD 1.26).
Strengths and limitations: This is the first longitudinal study demonstrating the feasibility of a DCP for patients with acute MSK conditions involving several body areas. Major strengths of this study are the large sample size, the wide range of MSK conditions studied, the breadth of outcomes measured, and the very high retention rate and adherence level. The major limitation regards to the absence of a control group.
Conclusions: We observed very high completion and engagement rates, as well as clinically relevant changes in all health-related outcomes and productivity recovery. We believe this DCP holds great potential in the delivery of effective and scalable MSK care.
Trial registration: NCT, NCT04092946 . Registered 17/09/2019.
Keywords: Digital therapy; Home-based digital rehabilitation; Musculoskeletal pain; Physical therapy; Rehabilitation; eHealth.
© 2021. The Author(s).
Conflict of interest statement
Fernando Correia, Fabíola Costa, Maria Molinos, Dora Janela and Virgílio Bento are employees at SWORD Health, the study sponsor. Gerard Francisco and Jorge Lains received a scientific advisor honorarium from SWORD Health.
Figures
Similar articles
-
Engagement and Utilization of a Complete Remote Digital Care Program for Musculoskeletal Pain Management in Urban and Rural Areas Across the United States: Longitudinal Cohort Study.JMIR Mhealth Uhealth. 2023 Mar 16;11:e44316. doi: 10.2196/44316. JMIR Mhealth Uhealth. 2023. PMID: 36735933 Free PMC article.
-
Asynchronous and Tailored Digital Rehabilitation of Chronic Shoulder Pain: A Prospective Longitudinal Cohort Study.J Pain Res. 2022 Jan 8;15:53-66. doi: 10.2147/JPR.S343308. eCollection 2022. J Pain Res. 2022. PMID: 35035234 Free PMC article.
-
Impacts of Digital Care Programs for Musculoskeletal Conditions on Depression and Work Productivity: Longitudinal Cohort Study.J Med Internet Res. 2022 Jul 25;24(7):e38942. doi: 10.2196/38942. J Med Internet Res. 2022. PMID: 35714099 Free PMC article.
-
A systematic review and evidence synthesis of non-medical triage, self-referral and direct access services for patients with musculoskeletal pain.PLoS One. 2020 Jul 6;15(7):e0235364. doi: 10.1371/journal.pone.0235364. eCollection 2020. PLoS One. 2020. PMID: 32628696 Free PMC article.
-
Benchmarking community/primary care musculoskeletal services: A narrative review and recommendation.Musculoskeletal Care. 2023 Mar;21(1):148-158. doi: 10.1002/msc.1676. Epub 2022 Aug 11. Musculoskeletal Care. 2023. PMID: 35957541 Review.
Cited by
-
The potential of a multimodal digital care program in addressing healthcare inequities in musculoskeletal pain management.NPJ Digit Med. 2023 Oct 10;6(1):188. doi: 10.1038/s41746-023-00936-2. NPJ Digit Med. 2023. PMID: 37816899 Free PMC article.
-
Managing Musculoskeletal Pain in Older Adults Through a Digital Care Solution: Secondary Analysis of a Prospective Clinical Study.JMIR Rehabil Assist Technol. 2023 Aug 15;10:e49673. doi: 10.2196/49673. JMIR Rehabil Assist Technol. 2023. PMID: 37465960 Free PMC article.
-
Digital Care Programs for Chronic Hip Pain: A Prospective Longitudinal Cohort Study.Healthcare (Basel). 2022 Aug 22;10(8):1595. doi: 10.3390/healthcare10081595. Healthcare (Basel). 2022. PMID: 36011251 Free PMC article.
-
Fear Avoidance Beliefs in Upper-Extremity Musculoskeletal Pain Conditions: Secondary Analysis of a Prospective Clinical Study on Digital Care Programs.Pain Med. 2023 Apr 3;24(4):451-460. doi: 10.1093/pm/pnac149. Pain Med. 2023. PMID: 36200858 Free PMC article.
-
Engagement and Utilization of a Complete Remote Digital Care Program for Musculoskeletal Pain Management in Urban and Rural Areas Across the United States: Longitudinal Cohort Study.JMIR Mhealth Uhealth. 2023 Mar 16;11:e44316. doi: 10.2196/44316. JMIR Mhealth Uhealth. 2023. PMID: 36735933 Free PMC article.
References
-
- United States Bone and Joint Initiative:The Burden of Musculoskeletal Diseases in the United States (BMUS), Third Edition [http://www.boneandjointburden.org].
-
- Abareshi F, Yarahmadi R, Solhi M, Farshad AA. Educational intervention for reducing work-related musculoskeletal disorders and promoting productivity. Int J Occup Saf Ergon. 2015;21(4):480–485. - PubMed
-
- Platts-Mills TF, McLean SA, Weinberger M, Stearns SC, Bush M, Teresi BB, Hurka-Richardson K, Kroenke K, Kerns RD, Weaver MA, et al. Brief educational video plus telecare to enhance recovery for older emergency department patients with acute musculoskeletal pain: study protocol for the BETTER randomized controlled trial. Trials. 2020;21(1):615. - PMC - PubMed
-
- Luque-Suarez A, Martinez-Calderon J, Falla D. Role of kinesiophobia on pain, disability and quality of life in people suffering from chronic musculoskeletal pain: a systematic review. Br J Sports Med. 2019;53(9):554–559. - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
