

Respiratory effects of lung recruitment maneuvers depend on the recruitment-to-inflation ratio in patients with COVID-19-related acute respiratory distress syndrome
- PMID: 34983597
- PMCID: PMC8727044
- DOI: 10.1186/s13054-021-03876-z
Respiratory effects of lung recruitment maneuvers depend on the recruitment-to-inflation ratio in patients with COVID-19-related acute respiratory distress syndrome
Abstract
Background: In the context of acute respiratory distress syndrome (ARDS), the response to lung recruitment maneuvers (LRMs) varies considerably from one patient to another and so is difficult to predict. The aim of the study was to determine whether or not the recruitment-to-inflation (R/I) ratio could differentiate between patients according to the change in lung mechanics during the LRM.
Methods: We evaluated the changes in gas exchange and respiratory mechanics induced by a stepwise LRM at a constant driving pressure of 15 cmH2O during pressure-controlled ventilation. We assessed lung recruitability by measuring the R/I ratio. Patients were dichotomized with regard to the median R/I ratio.
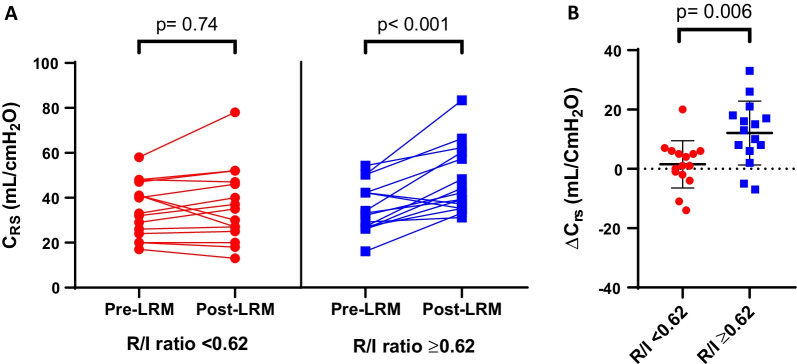
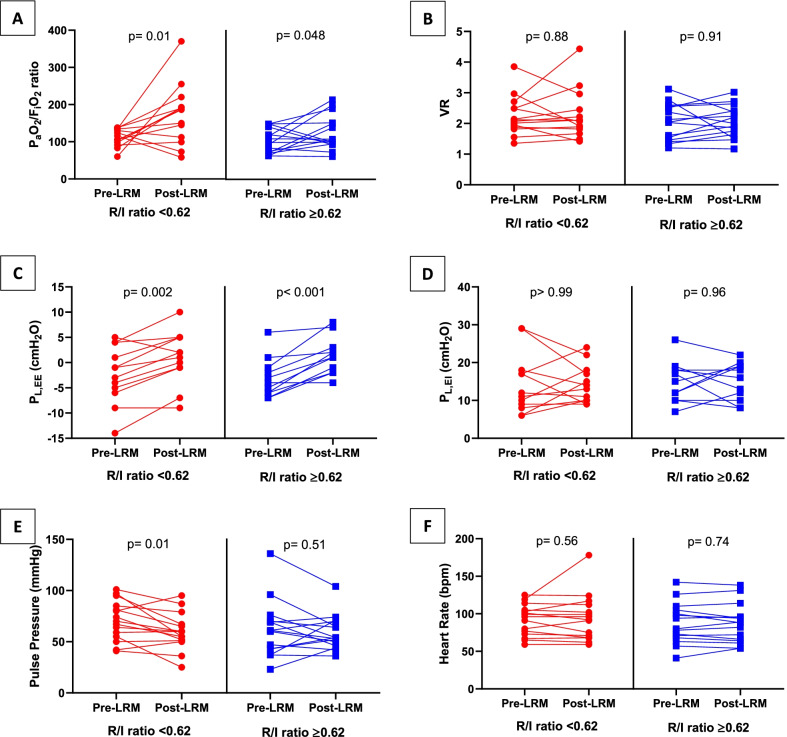
Results: We included 30 patients with moderate-to-severe ARDS and a median [interquartile range] R/I ratio of 0.62 [0.42-0.83]. After the LRM, patients with high recruitability (R/I ratio ≥ 0.62) presented an improvement in the PaO2/FiO2 ratio, due to significant increase in respiratory system compliance (33 [27-42] vs. 42 [35-60] mL/cmH2O; p < 0.001). In low recruitability patients (R/I < 0.62), the increase in PaO2/FiO2 ratio was associated with a significant decrease in pulse pressure as a surrogate of cardiac output (70 [55-85] vs. 50 [51-67] mmHg; p = 0.01) but not with a significant change in respiratory system compliance (33 [24-47] vs. 35 [25-47] mL/cmH2O; p = 0.74).
Conclusion: After the LRM, patients with high recruitability presented a significant increase in respiratory system compliance (indicating a gain in ventilated area), while those with low recruitability presented a decrease in pulse pressure suggesting a drop in cardiac output and therefore in intrapulmonary shunt.
Keywords: Acute respiratory distress syndrome; Mechanical ventilation; Recruitability; Recruitment maneuver; Respiratory mechanics.
© 2022. The Author(s).
Conflict of interest statement
The authors report no disclosures of relevance to the manuscript.
Figures
References
-
- ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307:2526–33. - PubMed
-
- Acute Respiratory Distress Syndrome Network, Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–8. - PubMed
-
- Meade MO, Cook DJ, Guyatt GH, Slutsky AS, Arabi YM, Cooper DJ, et al. Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2008;299:637. doi: 10.1001/jama.299.6.637. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
