

Long-term outcome of percutaneous radiofrequency ablation for periportal hepatocellular carcinoma: tumor recurrence or progression, survival and clinical significance
- PMID: 34983650
- PMCID: PMC8725335
- DOI: 10.1186/s40644-021-00442-2
Long-term outcome of percutaneous radiofrequency ablation for periportal hepatocellular carcinoma: tumor recurrence or progression, survival and clinical significance
Abstract
Background/aim: Recent studies have suggested that periportal location of percutaneous radiofrequency ablation (RFA) for hepatocellular carcinoma (HCC) is considered as one of the independent risk factors for local tumor progression (LTP). However, the long-term therapeutic outcomes of percutaneous RFA as the first-line therapy for single periportal HCCand corresponding impacts on tumor recurrence or progression are still unclear.
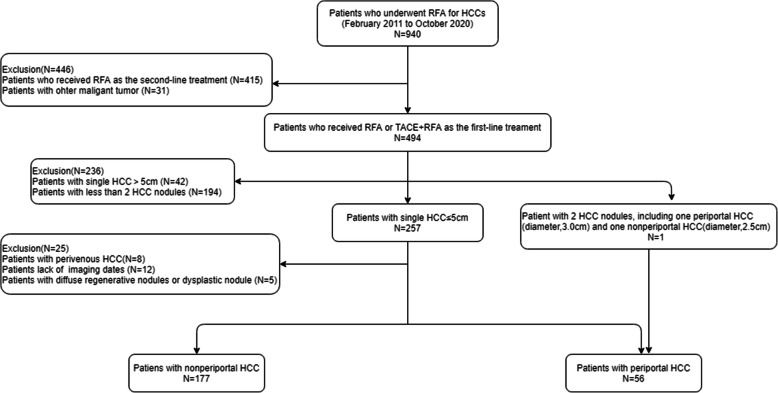
Materials and methods: From February 2011 to October 2020, a total of 233 patients with single nodular HCC ≤ 5 cm who underwent RFA ± transarterial chemoembolization (TACE) as first-line therapy was enrolled and analyzed, including 56 patients in the periportal group and 177 patients in the nonperiportal group. The long-term therapeutic outcomes between the two groups were compared, risk factors of tumor recurrence or progression were evaluated.
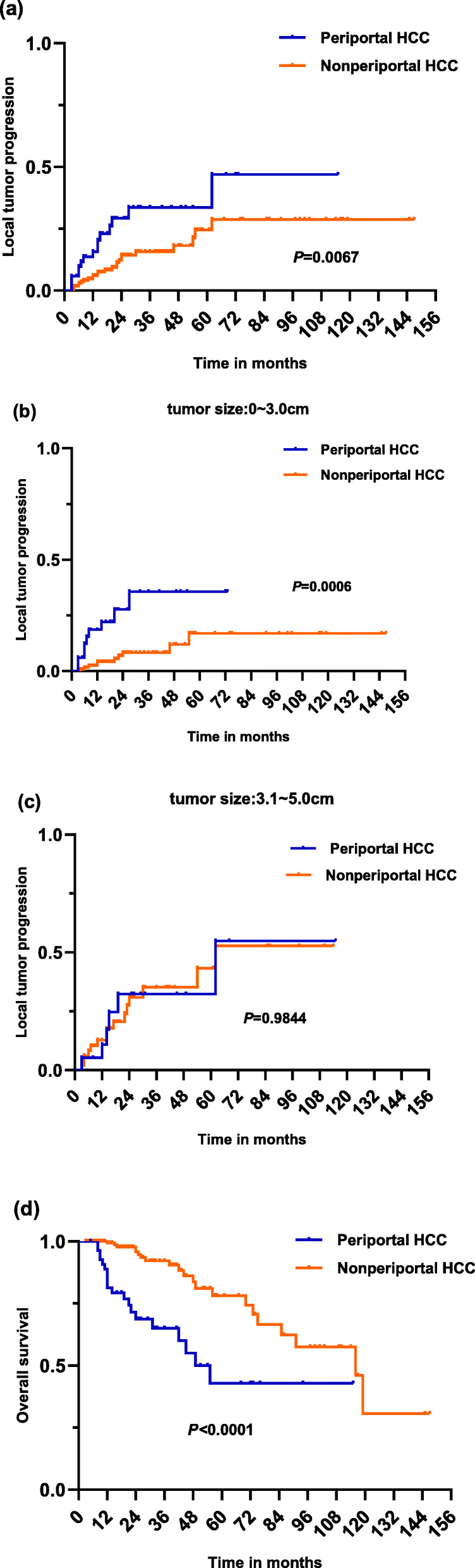
Results: The LTP rates at 1, 3, and 5 years were significantly higher in the periportal group than those in the nonperiportal group (15.7, 33.7, and 46.9% vs 6.0, 15.7, and 28.7%, respectively, P = 0.0067). The 1-, 3- and 5-year overall survival (OS) rates in the periportal group were significantly worse than those in the nonperiportal group (81.3, 65.1 and 42.9% vs 99.3, 90.4 and 78.1%, respectively, P<0.0001). In the subgroup of single HCC ≤ 3 cm, patients with periportal HCC showed significantly worse LTP P = 0.0006) and OS (P<0.0001) after RFA than patients with single nonperiportal HCC; The univariate and multivariate analyses revealed that tumor size, periportal HCC and AFP ≥ 400ug/ml were independent prognostic factors for tumor progression after RFA. Furthermore, patients with single periportal HCC had significantly higher risk for IDR(P = 0.0012), PVTT(P<0.0001) and extrahepatic recurrence(P = 0.0010) after RFA than those patients with single nonperiportal HCC. .
Conclusion: The long-term therapeutic outcomes of RFA as the first-line therapy for single periportal HCC were worse than those for single nonperiportal HCC, an increased higher risk of tumor recurrence or progression after RFA was significantly associated with periportal HCC.
Keywords: Hepatocellular carcinoma (HCC); Periportal; Radiofrequency ablation (RFA); Therapeutic outcomes; Tumor progression; Tumor recurrence.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing financial interests.
Figures


References
-
- Marrero JA, Kulik LM, Sirlin CB, Zhu AX, Finn RS, Abecassis MM, Roberts LR, Heimbach JK. Diagnosis, staging, and Management of Hepatocellular Carcinoma: 2018 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68(2):723–750. doi: 10.1002/hep.29913. - DOI - PubMed
-
- Shiina S, Tateishi R, Arano T, Uchino K, Enooku K, Nakagawa H, Asaoka Y, Sato T, Masuzaki R, Kondo Y, Goto T, Yoshida H, Omata M, Koike K. Radiofrequency ablation for hepatocellular carcinoma: 10-year outcome and prognostic factors. Am J Gastroenterol. 2012;107(4):569–577. doi: 10.1038/ajg.2011.425. - DOI - PMC - PubMed
-
- Kim YS, Lim HK, Rhim H, Lee MW, Choi D, Lee WJ, Paik SW, Koh KC, Lee JH, Choi MS, Gwak GY, Yoo BC. Ten-year outcomes of percutaneous radiofrequency ablation as first-line therapy of early hepatocellular carcinoma: analysis of prognostic factors. J Hepatol. 2013;58(1):89–97. doi: 10.1016/j.jhep.2012.09.020. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
