

Assessment and treatment of thyroid disorders in pregnancy and the postpartum period
- PMID: 34983968
- PMCID: PMC9020832
- DOI: 10.1038/s41574-021-00604-z
Assessment and treatment of thyroid disorders in pregnancy and the postpartum period
Abstract
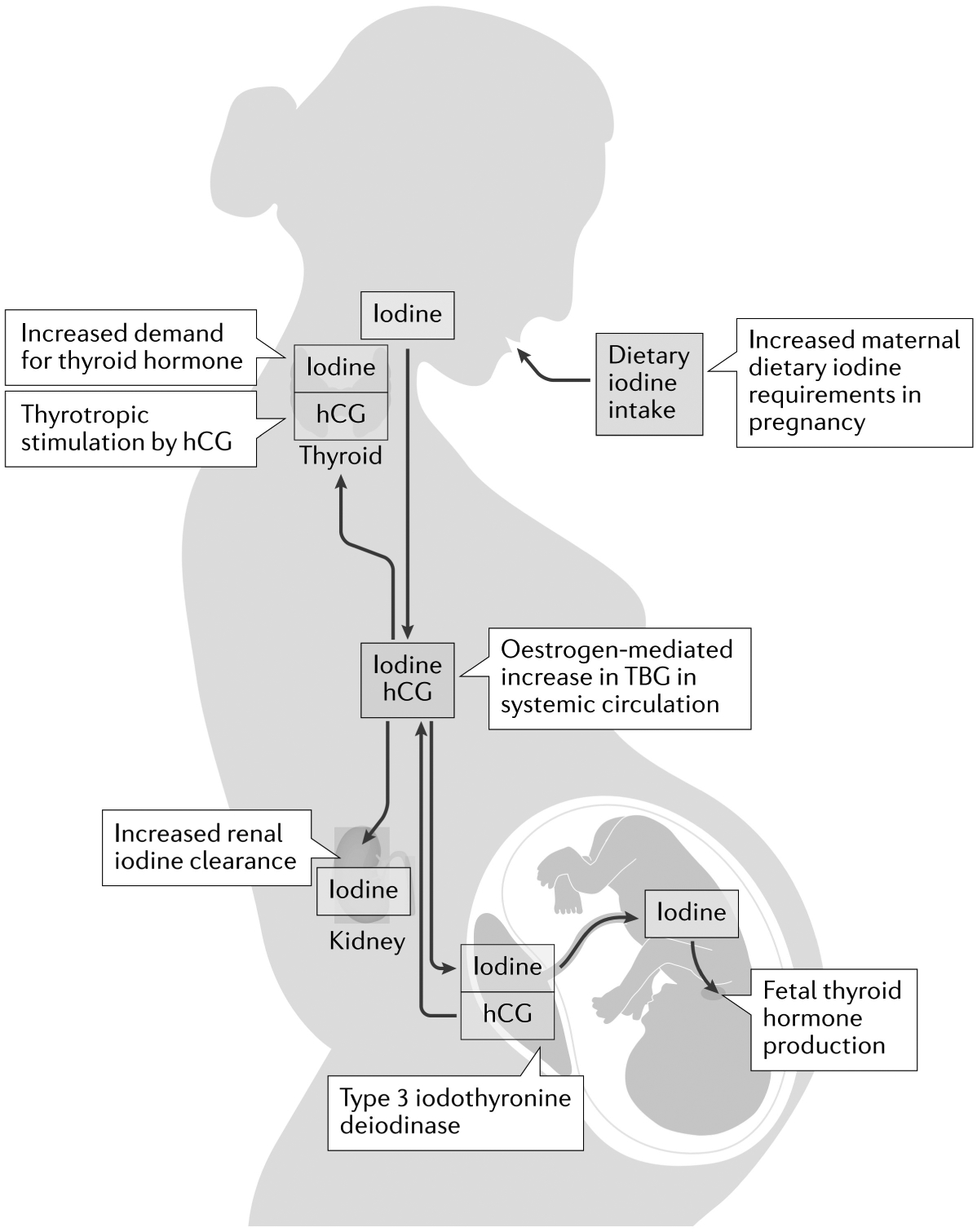
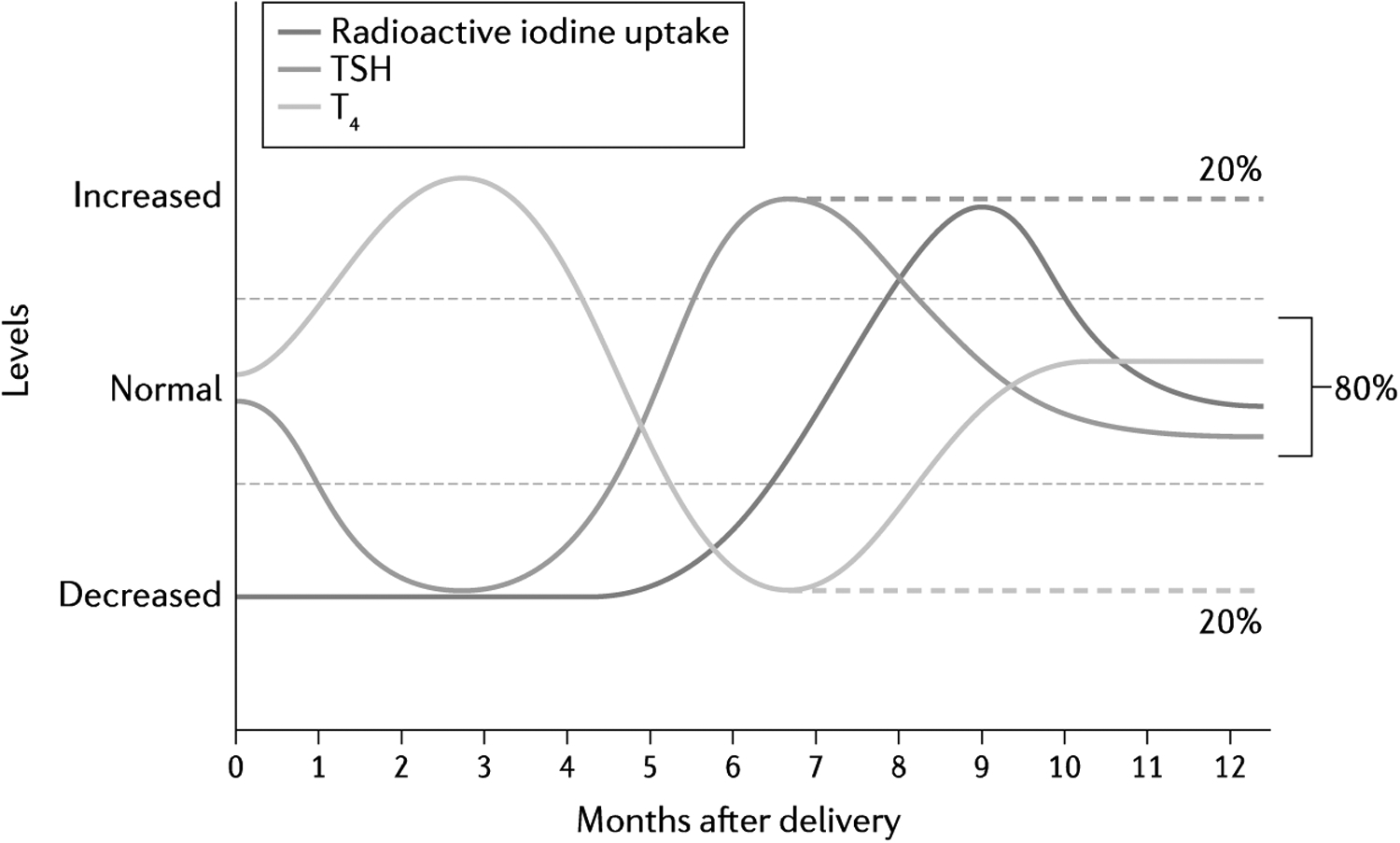
Thyroid disorders are prevalent in pregnant women. Furthermore, thyroid hormone has a critical role in fetal development and thyroid dysfunction can adversely affect obstetric outcomes. Thus, the appropriate management of hyperthyroidism, most commonly caused by Graves disease, and hypothyroidism, which in iodine sufficient regions is most commonly caused by Hashimoto thyroiditis, in pregnancy is important for the health of both pregnant women and their offspring. Gestational transient thyrotoxicosis can also occur during pregnancy and should be differentiated from Graves disease. Effects of thyroid autoimmunity and subclinical hypothyroidism in pregnancy remain controversial. Iodine deficiency is the leading cause of hypothyroidism worldwide. Despite global efforts to eradicate iodine deficiency disorders, pregnant women remain at risk of iodine deficiency due to increased iodine requirements during gestation. The incidence of thyroid cancer is increasing worldwide, including in young adults. As such, the diagnosis of thyroid nodules or thyroid cancer during pregnancy is becoming more frequent. The evaluation and management of thyroid nodules and thyroid cancer in pregnancy pose a particular challenge. Postpartum thyroiditis can occur up to 1 year after delivery and must be differentiated from other forms of thyroid dysfunction, as treatment differs. This Review provides current evidence and recommendations for the evaluation and management of thyroid disorders in pregnancy and in the postpartum period.
© 2022. Springer Nature Limited.
Conflict of interest statement
Competing interests
The authors declare no competing interests.
Figures
References
-
- Taylor PN et al. Global epidemiology of hyperthyroidism and hypothyroidism. Nat. Rev. Endocrinol 14, 301–316 (2018). - PubMed
-
- Dong AC & Stagnaro-Green A Differences in diagnostic criteria mask the true prevalence of thyroid disease in pregnancy: a systematic review and meta-analysis. Thyroid 29, 278–289 (2019). - PubMed
-
- Burrow GN, Fisher DA & Larsen PR Maternal and fetal thyroid function. N. Engl. J. Med 331, 1072–1078 (1994). - PubMed
-
- Stagnaro-Green A Approach to the patient with postpartum thyroiditis. J. Clin. Endocrinol. Metab 97, 334–342 (2012). - PubMed
-
- Yoshimura M & Hershman JM Thyrotropic action of human chorionic gonadotropin. Thyroid 5, 425–434 (1995). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
