

Accelerated orthodontic tooth movement: surgical techniques and the regional acceleratory phenomenon
- PMID: 34984554
- PMCID: PMC8727645
- DOI: 10.1186/s40902-021-00331-5
Accelerated orthodontic tooth movement: surgical techniques and the regional acceleratory phenomenon
Abstract
Background: Techniques to accelerate tooth movement have been a topic of interest in orthodontics over the past decade. As orthodontic treatment time is linked to potential detrimental effects, such as increased decalcification, dental caries, root resorption, and gingival inflammation, the possibility of reducing treatment time in orthodontics may provide multiple benefits to the patient. Another reason for the surge in interest in accelerated tooth movement has been the increased interest in adult orthodontics.
Review: This review summarizes the different methods for surgical acceleration of orthodontic tooth movement. It also describes the advantages and limitations of these techniques, including guidance for future investigations.
Conclusions: Optimization of the described techniques is still required, but some of the techniques appear to offer the potential for accelerating orthodontic tooth movement and improving outcomes in well-selected cases.
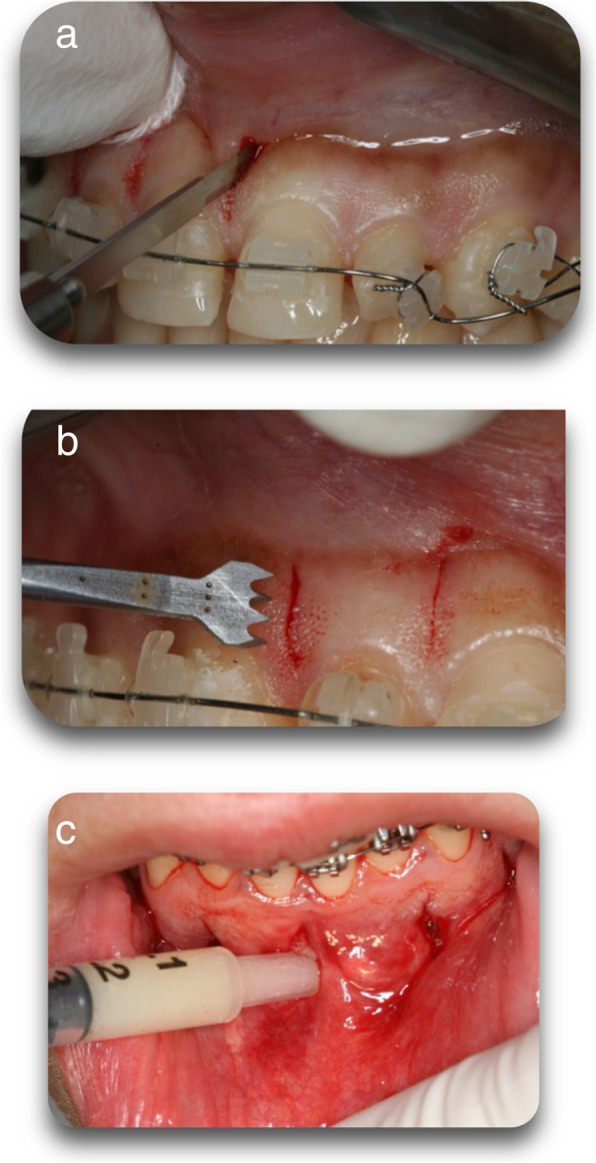
Keywords: Corticision; Microosteoperforations; Periodontally accelerated osteogenic orthodontics (PAOO); Piezocision; Regional acceleratory phenomenon.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures








Similar articles
-
Accelerating the Orthodontic Treatment Using Periodontally Accelerated Osteogenic Orthodontics (PAOO): A Periodontic-Orthodontic Interrelationship.Cureus. 2024 Jun 12;16(6):e62216. doi: 10.7759/cureus.62216. eCollection 2024 Jun. Cureus. 2024. PMID: 39006705 Free PMC article.
-
Periodontally accelerated osteogenic orthodontics (PAOO) - a review.J Clin Exp Dent. 2012 Dec 1;4(5):e292-6. doi: 10.4317/jced.50822. eCollection 2012 Dec 1. J Clin Exp Dent. 2012. PMID: 24455038 Free PMC article. Review.
-
Research progress in periodontally accelerated osteogenic orthodontics.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2024 Dec 28;49(12):2005-2015. doi: 10.11817/j.issn.1672-7347.2024.240345. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2024. PMID: 40195674 Free PMC article. Review. Chinese, English.
-
The Effectiveness of Periodontally Accelerated Osteogenic Orthodontics (PAOO) in Accelerating Tooth Movement and Supporting Alveolar Bone Thickness During Orthodontic Treatment: A Systematic Review.Cureus. 2022 May 14;14(5):e24985. doi: 10.7759/cureus.24985. eCollection 2022 May. Cureus. 2022. PMID: 35582021 Free PMC article. Review.
-
[Periodontally accelerated osteogenic orthodontics in clinical treatment].Zhonghua Kou Qiang Yi Xue Za Zhi. 2021 Oct 9;56(10):978-982. doi: 10.3760/cma.j.cn112144-20210726-00339. Zhonghua Kou Qiang Yi Xue Za Zhi. 2021. PMID: 34619890 Chinese.
Cited by
-
MicroRNA-155 targets SOCS1 to inhibit osteoclast differentiation during orthodontic tooth movement.BMC Oral Health. 2023 Dec 1;23(1):955. doi: 10.1186/s12903-023-03443-8. BMC Oral Health. 2023. PMID: 38041017 Free PMC article.
-
The osteogenic effect of 3D-printed bone grafting guides in PAOO: a retrospective cohort study.BMC Oral Health. 2025 Sep 2;25(1):1398. doi: 10.1186/s12903-025-06753-1. BMC Oral Health. 2025. PMID: 40898183 Free PMC article.
-
Use of Orthodontic Mini-Implants in Conjunction with Elastics for Extrusion of Impacted Canines and Correction of Bimaxillary Protrusion.J Pharm Bioallied Sci. 2024 Jul;16(Suppl 3):S2864-S2867. doi: 10.4103/jpbs.jpbs_581_24. Epub 2024 Jul 1. J Pharm Bioallied Sci. 2024. PMID: 39346131 Free PMC article.
-
The transparency of reporting 'harms' encountered with the surgically assisted acceleration of orthodontic tooth movement in the published randomized controlled trials: a meta-epidemiological study.Prog Orthod. 2023 Mar 21;24(1):11. doi: 10.1186/s40510-023-00457-4. Prog Orthod. 2023. PMID: 36941520 Free PMC article. Review.
-
Comparison of conventional orthodontic method with corticotomy and piezocision during rapid canine retraction.Bioinformation. 2025 Mar 31;21(3):324-328. doi: 10.6026/973206300210324. eCollection 2025. Bioinformation. 2025. PMID: 40599959 Free PMC article.
References
-
- Keim RG, Gottlieb EL, Nelson AH, Vogels DS. JCO orthodontic practice study. Part 1 Trends. J Clin Orthod. 2013;47(11):661–680. - PubMed
-
- https://us.dental-tribune.com/news/adults-are-seeking-orthodontic-treatm.... Accessed Sept 2021.
Publication types
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous