

Impact of COVID-19 on in-hospital cardiac arrest outcomes: An updated meta-analysis
- PMID: 34985120
- PMCID: PMC8747824
- DOI: 10.5603/CJ.a2021.0168
Impact of COVID-19 on in-hospital cardiac arrest outcomes: An updated meta-analysis
Abstract
Background: The main purposes of this meta-analysis are to update the information about the impact of coronavirus disease 2019 (COVID-19) pandemic on outcomes of in-hospital cardiac arrest (IHCA) and to investigate the impact of being infected by by severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2) on IHCA outcomes.
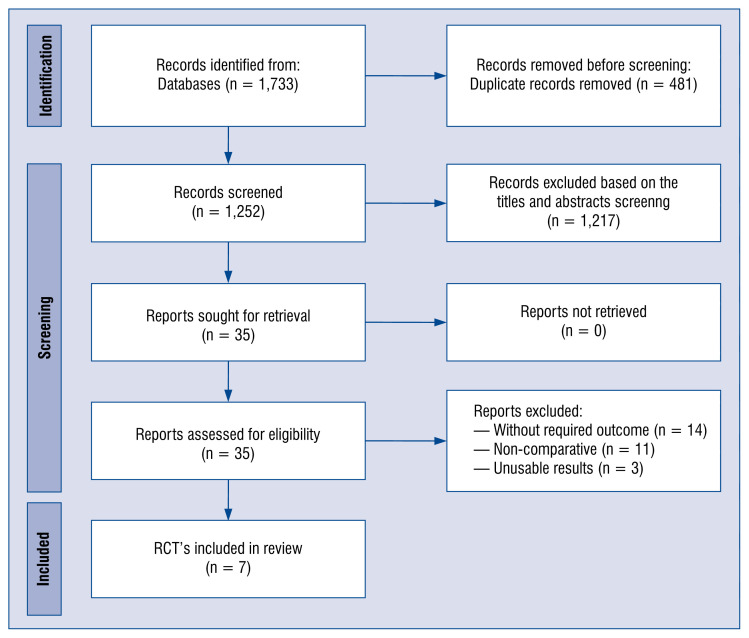
Methods: The current meta-analysis is an update and follows the recommendations of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
Results: In analyses, pre- and intra-COVID-19 periods were observed for: shockable rhythms in 17.6% vs. 16.2% (odds ratio [OR]: 1.11; 95% confidence interval [CI]: 0.71-1.72; p = 0.65), return of spontaneous circulation (ROSC) in 47.4% vs. 44.0% (OR: 1.36; 95% CI: 0.90-2.07; p = 0.15), 30-day mortality in 59.8% vs. 60.9% (OR: 0.95; 95% CI: 0.75-1.22; p = 0.69) and overall mortality 75.8% vs. 74.7% (OR: 0.80; 95% CI: 0.49-1.28; p = 0.35), respectively. In analyses, SARS-CoV-2 positive and negative patients were observed for: shockable rhythms in 9.6% vs. 19.8% (OR: 0.51; 95% CI: 0.35-0.73; p < 0.001), ROSC in 33.9% vs. 52.1% (OR: 0.47; 95% CI: 0.30-0.73; p < 0.001), 30-day mortality in 77.2% vs. 59.7% (OR: 2.08; 95% CI: 1.28-3.38; p = 0.003) and overall mortality in 94.9% vs. 76.7% (OR: 3.20; 95% CI: 0.98-10.49; p = 0.05), respectively.
Conclusions: Despite ROSC, 30-day and overall mortality rate were not statistically different in pre- vs. intra-COVID-19 periods, a lower incidence of ROSC and higher 20-day mortality rate were observed in SARS-CoV-2 (+) compared to SARS-CoV-2 (-) patients.
Keywords: COVID-19; SARS-CoV-2; cardiopulmonary resuscitation; coronavirus disease 2019; in-hospital cardiac arrest; meta-analysis; outcome; pandemic.
Conflict of interest statement
Figures
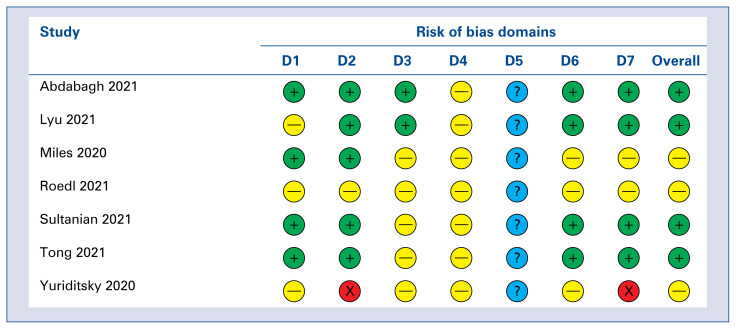
 Serious;
Serious;
 Moderate;
Moderate;
 Low;
Low;
 No information.
No information.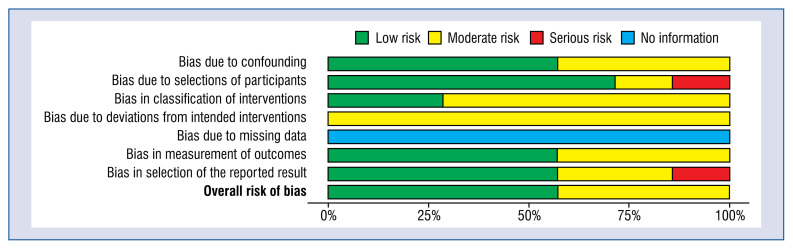
Comment in
-
Influence of COVID-19 on cardiac arrest outcomes.Cardiol J. 2023;30(1):163-164. doi: 10.5603/CJ.a2022.0114. Epub 2022 Nov 24. Cardiol J. 2023. PMID: 36420628 Free PMC article. No abstract available.
Similar articles
-
Uncovering the effects of COVID-19 on in-hospital cardiac arrest - a living systematic review and meta-analysis.Ann Agric Environ Med. 2023 Sep 28;30(3):498-504. doi: 10.26444/aaem/166757. Epub 2023 Jun 16. Ann Agric Environ Med. 2023. PMID: 37772526
-
Effects of COVID-19 on in-hospital cardiac arrest: incidence, causes, and outcome - a retrospective cohort study.Scand J Trauma Resusc Emerg Med. 2021 Feb 8;29(1):30. doi: 10.1186/s13049-021-00846-w. Scand J Trauma Resusc Emerg Med. 2021. PMID: 33557923 Free PMC article.
-
Outcomes of out-of-hospital cardiac arrest in patients with SARS-CoV-2 infection: a systematic review and meta-analysis.Eur J Emerg Med. 2021 Dec 1;28(6):423-431. doi: 10.1097/MEJ.0000000000000878. Eur J Emerg Med. 2021. PMID: 34690258 Free PMC article.
-
Characteristics and outcomes of in-hospital cardiac arrest in COVID-19. A systematic review and meta-analysis.Cardiol J. 2021;28(4):503-508. doi: 10.5603/CJ.a2021.0043. Epub 2021 May 4. Cardiol J. 2021. PMID: 33942278 Free PMC article.
-
The Impact of COVID-19 on Pediatric Cardiac Arrest Outcomes: A Systematic Review and Meta-Analysis.Int J Environ Res Public Health. 2023 Jan 8;20(2):1104. doi: 10.3390/ijerph20021104. Int J Environ Res Public Health. 2023. PMID: 36673858 Free PMC article.
Cited by
-
Influence of COVID-19 on cardiac arrest outcomes.Cardiol J. 2023;30(1):163-164. doi: 10.5603/CJ.a2022.0114. Epub 2022 Nov 24. Cardiol J. 2023. PMID: 36420628 Free PMC article. No abstract available.
-
Impact of COVID-19 on Nonpulmonary Critical Illness: Prevalence, Clinical Manifestations, Management, and Outcomes.Clin Chest Med. 2023 Jun;44(2):249-262. doi: 10.1016/j.ccm.2022.11.011. Epub 2022 Nov 23. Clin Chest Med. 2023. PMID: 37085218 Free PMC article. Review.
-
Effect of Coronary Artery Disease on COVID-19-Prognosis and Risk Assessment: A Systematic Review and Meta-Analysis.Biology (Basel). 2022 Jan 29;11(2):221. doi: 10.3390/biology11020221. Biology (Basel). 2022. PMID: 35205088 Free PMC article.
-
Assessing Key Factors Influencing Successful Resuscitation Outcomes in Out-of-Hospital Cardiac Arrest (OHCA).J Clin Med. 2024 Dec 4;13(23):7399. doi: 10.3390/jcm13237399. J Clin Med. 2024. PMID: 39685857 Free PMC article.
-
Outcome of In-Hospital Cardiac Arrest among Patients with COVID-19: A Systematic Review and Meta-Analysis.J Clin Med. 2023 Apr 10;12(8):2796. doi: 10.3390/jcm12082796. J Clin Med. 2023. PMID: 37109134 Free PMC article. Review.
References
-
- Rodriguez-Morales AJ, Bonilla-Aldana DK, Balbin-Ramon GJ, et al. History is repeating itself: Probable zoonotic spillover as the cause of the 2019 novel Coronavirus Epidemic. Infez Med. 2020;28(1):3–5. - PubMed
-
- Attila K, Ludwin K, Evrin T, et al. The impact of COVID-19 on airway management in prehospital resuscitation. Dis Emerg Med J. 2020;5(4):216–217. doi: 10.5603/demj.a2020.0047.. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
