

Direct Oral Anticoagulants Versus Warfarin in Patients With Atrial Fibrillation: Patient-Level Network Meta-Analyses of Randomized Clinical Trials With Interaction Testing by Age and Sex
- PMID: 34985309
- PMCID: PMC8800560
- DOI: 10.1161/CIRCULATIONAHA.121.056355
Direct Oral Anticoagulants Versus Warfarin in Patients With Atrial Fibrillation: Patient-Level Network Meta-Analyses of Randomized Clinical Trials With Interaction Testing by Age and Sex
Erratum in
-
Correction to: Direct Oral Anticoagulants Versus Warfarin in Patients With Atrial Fibrillation: Patient-Level Network Meta-Analyses of Randomized Clinical Trials With Interaction Testing by Age and Sex.Circulation. 2022 Feb 22;145(8):e640. doi: 10.1161/CIR.0000000000001058. Epub 2022 Feb 21. Circulation. 2022. PMID: 35188800 No abstract available.
Abstract
Background: Direct oral anticoagulants (DOACs) are preferred over warfarin for stroke prevention in atrial fibrillation. Meta-analyses using individual patient data offer substantial advantages over study-level data.
Methods: We used individual patient data from the COMBINE AF (A Collaboration Between Multiple Institutions to Better Investigate Non-Vitamin K Antagonist Oral Anticoagulant Use in Atrial Fibrillation) database, which includes all patients randomized in the 4 pivotal trials of DOACs versus warfarin in atrial fibrillation (RE-LY [Randomized Evaluation of Long-Term Anticoagulation Therapy], ROCKET AF [Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared With Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation], ARISTOTLE [Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation], and ENGAGE AF-TIMI 48 [Effective Anticoagulation With Factor Xa Next Generation in Atrial Fibrillation-Thrombolysis in Myocardial Infarction 48]), to perform network meta-analyses using a stratified Cox model with random effects comparing standard-dose DOAC, lower-dose DOAC, and warfarin. Hazard ratios (HRs [95% CIs]) were calculated for efficacy and safety outcomes. Covariate-by-treatment interaction was estimated for categorical covariates and for age as a continuous covariate, stratified by sex.
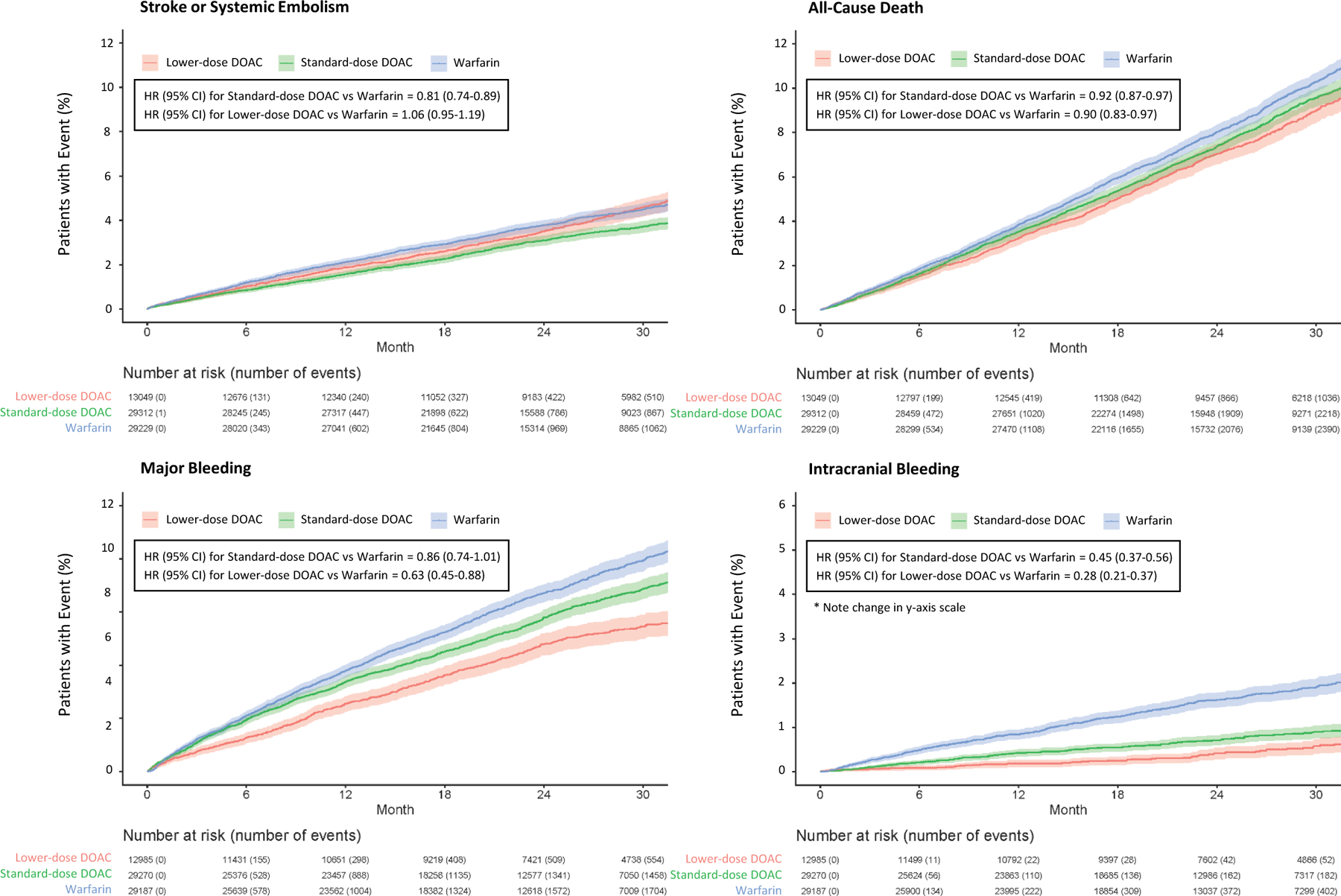
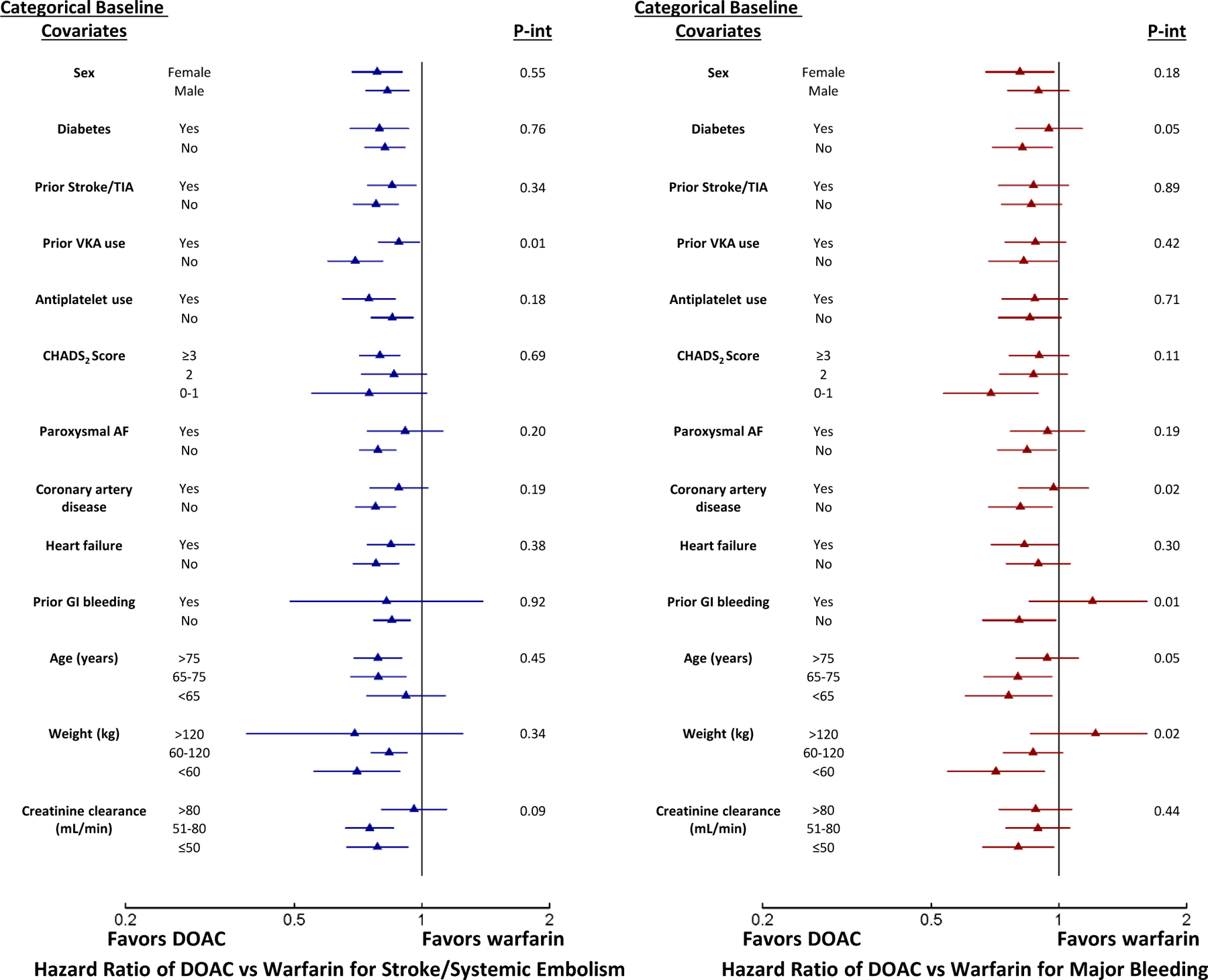
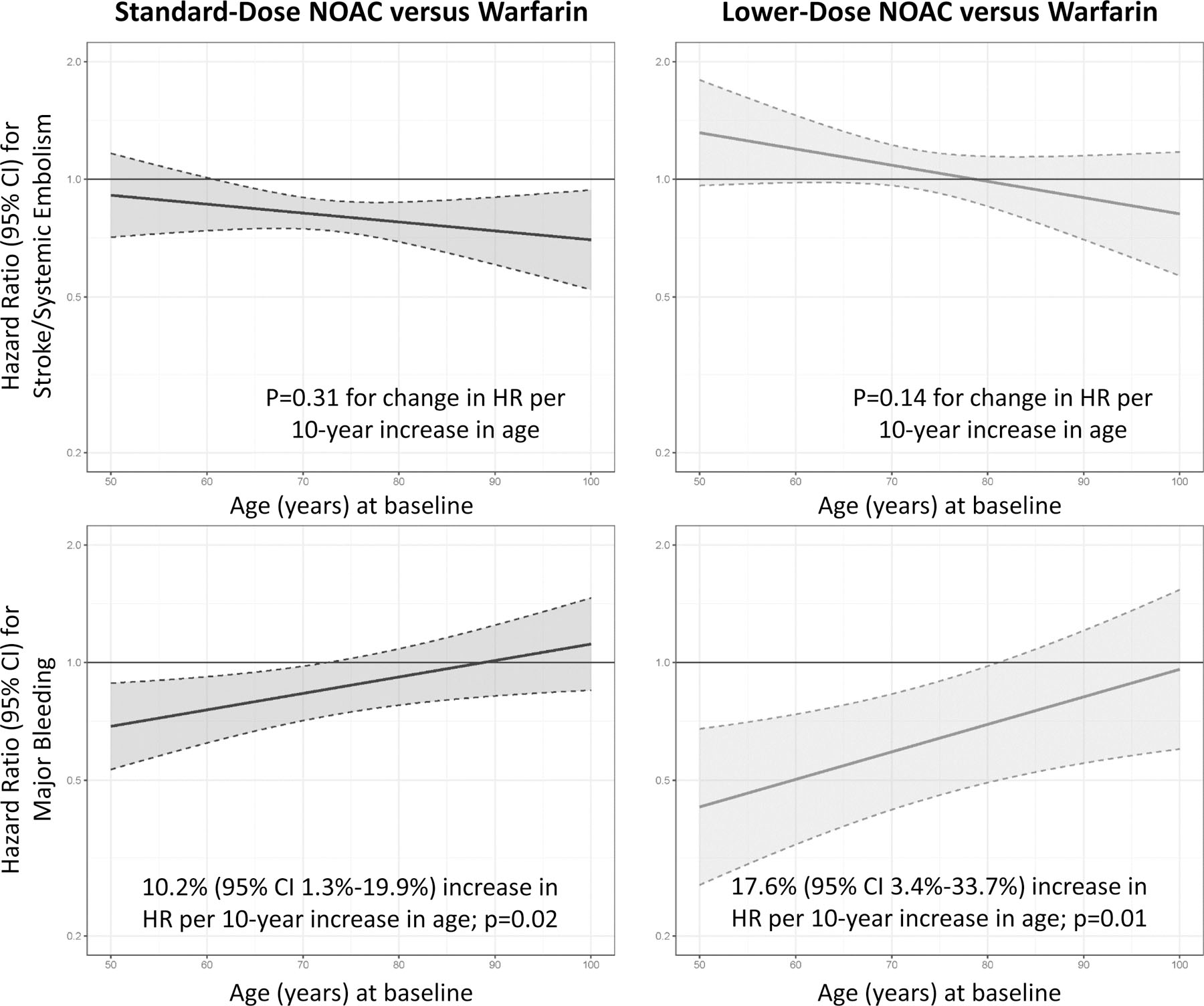
Results: A total of 71 683 patients were included (29 362 on standard-dose DOAC, 13 049 on lower-dose DOAC, and 29 272 on warfarin). Compared with warfarin, standard-dose DOACs were associated with a significantly lower hazard of stroke or systemic embolism (883/29 312 [3.01%] versus 1080/29 229 [3.69%]; HR, 0.81 [95% CI, 0.74-0.89]), death (2276/29 312 [7.76%] versus 2460/29 229 [8.42%]; HR, 0.92 [95% CI, 0.87-0.97]), and intracranial bleeding (184/29 270 [0.63%] versus 409/29 187 [1.40%]; HR, 0.45 [95% CI, 0.37-0.56]), but no statistically different hazard of major bleeding (1479/29 270 [5.05%] versus 1733/29 187 [5.94%]; HR, 0.86 [95% CI, 0.74-1.01]), whereas lower-dose DOACs were associated with no statistically different hazard of stroke or systemic embolism (531/13 049 [3.96%] versus 1080/29 229 [3.69%]; HR, 1.06 [95% CI, 0.95-1.19]) but a lower hazard of intracranial bleeding (55/12 985 [0.42%] versus 409/29 187 [1.40%]; HR, 0.28 [95% CI, 0.21-0.37]), death (1082/13 049 [8.29%] versus 2460/29 229 [8.42%]; HR, 0.90 [95% CI, 0.83-0.97]), and major bleeding (564/12 985 [4.34%] versus 1733/29 187 [5.94%]; HR, 0.63 [95% CI, 0.45-0.88]). Treatment effects for standard- and lower-dose DOACs versus warfarin were consistent across age and sex for stroke or systemic embolism and death, whereas standard-dose DOACs were favored in patients with no history of vitamin K antagonist use (P=0.01) and lower creatinine clearance (P=0.09). For major bleeding, standard-dose DOACs were favored in patients with lower body weight (P=0.02). In the continuous covariate analysis, younger patients derived greater benefits from standard-dose (interaction P=0.02) and lower-dose DOACs (interaction P=0.01) versus warfarin.
Conclusions: Compared with warfarin, DOACs have more favorable efficacy and safety profiles among patients with atrial fibrillation.
Keywords: anticoagulants; atrial fibrillation; meta-analysis; stroke; warfarin.
Conflict of interest statement
Conflict of Interest Disclosures
APC reports grants from National Institutes of Health, during the conduct of the study. HH has nothing to disclose. SJC reports personal fees from BMS, personal fees from Bayer, personal fees from Boehringer Ingelheim, personal fees from daiichi Sankyo, personal fees from Portola, during the conduct of the study. JE reports honoraria and grant support from Astra Zeneca, Bayer, Boehringer Ingelheim, Bristol-Myers-Squibb/Pfizer, Daiichi Sankyo, Glaxo Smith Kline, Janssen, sanofi aventis and Eli Lilly as well as a personnel award from the Heart and Stroke Foundation. RPG reports personal fees from Amarin, personal fees from American College of Cardiology, grants and personal fees from Amgen, grants from Anthos Therapeutics, personal fees from AstraZeneca, personal fees from Boehringer-Ingelheim, personal fees from Bristol-Myers-Squibb, personal fees from CryoLife, personal fees from CVS Caremark, grants and personal fees from Daiichi-Sankyo, personal fees from Dr. Reddy’s Laboratories, personal fees from Eli Lilly and Company, personal fees from Esperion, personal fees from Gilead, personal fees from GlaxoSmithKline, personal fees from Janssen, personal fees from Lexicon, grants and personal fees from Merck, personal fees from Pfizer, personal fees from St. Lukes, personal fees from SAJA Pharmaceuticals, personal fees from Samsung, personal fees from Servier, outside the submitted work. DAM reports being member of the TIMI Study Group which has received institutional research grant support through Brigham and Women’s Hospital from: Abbott, Amgen, Anthos Therapeutics, AstraZeneca, Bayer HealthCare Pharmaceuticals, Inc., Daiichi-Sankyo, Eisai, Intarcia, MedImmune, Merck, Novartis, Pfizer, Quark Pharmaceuticals, Regeneron Pharmaceuticals, Inc., Roche, Siemens Healthcare Diagnostics, Inc., The Medicines Company, Zora Biosciences. MRP reports grants from ASTRA ZENECA, grants from BAYER, personal fees from BAYER, grants from JANSSEN, personal fees from JANSSEN, personal fees from MYTONOMY, grants from PROCYRION, personal fees from PROCYRION, grants from HEARTFLOW, outside the submitted work. LW reports grants from AstraZeneca, grants from Boehringer Ingelheim, grants from Bristol-Myers Squibb/Pfizer, grants from GlaxoSmithKline, grants from Merck & Co., grants from Roche Diagnostics, personal fees from Abbot, outside the submitted work. JHA reports grants from Bayer, grants and personal fees from Bristol Myers Squibb, grants and personal fees from CryoLife, personal fees from Janssen, personal fees from Pfizer, personal fees from Portola, and grants from XaTek outside the submitted work. MCB reports other from Pfizer, other from VIFOR, other from CSL behring, outside the submitted work. APB has nothing to disclose. EAB reports being member of the TIMI Study Group which has received institutional research grant support through Brigham and Women’s Hospital from: Abbott, Amgen, Anthos Therapeutics, AstraZeneca, Bayer HealthCare Pharmaceuticals, Inc., Daiichi-Sankyo, Eisai, Intarcia, MedImmune, Merck, Novartis, Pfizer, Quark Pharmaceuticals, Regeneron Pharmaceuticals, Inc., Roche, Siemens Healthcare Diagnostics, Inc., The Medicines Company, Zora Biosciences. TFC has nothing to disclose. LD reports funding from Boehringer Ingelheim, during the conduct of the study. ME reports grants and other from Boehringer Ingelheim,, other from Sanofi – Aventis, other from Boston Scientific, other from Alta Thera, other from Anthos, other from Biogen Idec, other from Boston Scientific, grants from Pfizer, grants from J & J, grants from Daiichi Sankyo Pharma Development, during the conduct of the study. KAAF reports grants and personal fees from Bayer/Janssen, grants from AstraZeneca, personal fees from Verseon, outside the submitted work. BG has nothing to disclose. JLH reports personal fees from Boehringer Ingelheim, Bayer Healthcare, Ortho-McNeil-Janssen, Pfizer, Bristol Myers Squibb, and Daiichi Sankyo during the conduct of the study and personal fees from Boehringer Ingelheim, Ortho-McNeil Janssen, the ATLAS Group, Duke Clinical Research Institute and TIMI Group outside the submitted work. ZH reports consulting and lecture fees from Boehringer Ingelheim and Pfizer/BMS, grants from The Swedish Society for Medical Research (grant no. S17–0133) and The Swedish Heart-Lung Foundation (grant no. 20200722), during the conduct of the study; fees paid to his institution for advisory boards and lectures from Roche Diagnostics, outside the submitted work. SHH reports personal fees from BI, personal fees from BMS, personal fees from Pfizer, personal fees from Daiichi Sankyo, personal fees from Bayer Healthcare, personal fees from Medtronic, personal fees from sanofi, personal fees from zoll, outside the submitted work. KH has nothing to disclose. EH reports consulting fees from Anthos Therapeutics, Bristol Myers Squibb/Pfizer, Janssen, Medtronic, Honoraria from Boehringer Ingelheim, Bristol Myers Squibb/Pfizer, and Advisory Board fees from Anthos Therapeutics, CryoLife, outside of the submitted work. ETK reports personal fees from Daiichi-Sankyo, personal fees from AstraZeneca, personal fees from Bristol-Myers Squibb, grants and personal fees from Ono Pharmaceutical, personal fees from MSD KK, personal fees from Pfizer, from Tanabe-Mitsubishi, personal fees from Bayer, from Boehringer Ingelheim, grants from Abbott Japan, personal fees from Amgen, personal fees from Takeda, during the conduct of the study. JK reports grants from Daiichi-Sankyo, during the conduct of the study; and I am a member of the TIMI Study Group which has received institutional research grant support through Brigham and Women’s Hospital from: Abbott, Amgen, Anthos Therapeutics, AstraZeneca, Bayer HealthCare Pharmaceuticals, Inc., Daiichi-Sankyo, Eisai, Intarcia, MedImmune, Merck, Novartis, Pfizer, Quark Pharmaceuticals, Regeneron Pharmaceuticals, Inc., Roche, Siemens Healthcare Diagnostics, Inc., The Medicines Company, Zora Biosciences. RDL reports personal fees from Bayer, personal fees from Boehringer Ingleheim, grants from Bristol-Myers Squibb, personal fees from Bristol-Myers Squibb, personal fees from Daiichi Sankyo, personal fees from Glaxo Smith Kline, grants from Glaxo Smith Kline, personal fees from Medtronic, grants from Medtronic, personal fees from Merck, grants from Pfizer, personal fees from Pfizer, personal fees from Portola, personal fees from Sanofi, grants from Sanofi, outside the submitted work. KWM reports grants from Afferent, grants from AHA, grants and personal fees from Amgen, personal fees from Anthos, personal fees from Applied Therapeutics, grants from Apple, Inc, grants and personal fees from AstraZeneca, grants and personal fees from Bayer, grants from Cardiva Medical, Inc, personal fees from CSL Behring, grants from Eidos, personal fees from Elsevier, grants from Ferring, grants from Gilead, grants from Google (Verily), personal fees from Inova, personal fees from Intermountain Health, grants and personal fees from Johnson & Johnson, grants from Luitpold, personal fees from Medscape, grants from Medtronic, grants from Merck, personal fees from Mount Sinai, personal fees from Mundi Pharma, personal fees from Myokardia, grants and personal fees from Novartis, personal fees from Novo Nordisk, personal fees from Otsuka, personal fees from Portola, grants from Sanifit, grants and personal fees from Sanofi, personal fees from SmartMedics, grants from St. Jude, personal fees from Theravance, outside the submitted work. JO reports fees to his institution, for consultant/advisory boards (including study steering committees and data safety monitoring boards) and lectures, from Alexion, AstraZeneca, Bayer, BMS, Boehringer-Ingelheim, Daichii-Sankyo, Janssen, Novartis, Pfizer, Roche Diagnostics and Sanofi, outside the submitted work. JPP reports grants from Johnson & Johnson, during the conduct of the study; grants from Bayer, grants and personal fees from Boston Scientific, grants and personal fees from Abbott, personal fees from BMS, outside the submitted work. CTR reports grants from Daiichi Sankyo, during the conduct of the study; grants and personal fees from Anthos, grants and personal fees from Boehringer Ingelheim, grants from Daiichi Sankyo, grants from AstraZeneca, grants from National Institutes of Health, personal fees from Bayer, personal fees from Bristol Myers Squibb, personal fees from Janssen, personal fees from Pfizer, personal fees from Portola, outside the submitted work; and Ýr. Ruff is a member of the TIMI Study Group, which has received institutional research grant support through Brigham and Women’s Hospital from: Abbott, Amgen, Anthos Therapeutics, AstraZeneca, Bayer HealthCare Pharmaceuticals, Inc., Daiichi-Sankyo, Eisai, Intarcia, MedImmune, Merck, Novartis, Pfizer, Quark Pharmaceuticals, Regeneron Pharmaceuticals, Inc., Roche, Siemens Healthcare Diagnostics, Inc., The Medicines Company, Zora Biosciences. JS reports personal fees from Amgen, personal fees from Astra Zeneca, grants and personal fees from Bayer Healthcare, personal fees from Boehringer-Ingelheim, grants and personal fees from Biosense Webster, grants and personal fees from Boston Scientifc, personal fees from Bristol-Myers Squibb, grants and personal fees from Daiichi-Sankyo, grants and personal fees from Medtronic, personal fees from Novartis, personal fees from Pfizer, personal fees from Portola / Alexion, grants and personal fees from Abbott, other from CorXL, grants and personal fees from Biotronik, personal fees from Medscape, personal fees from WebMD, personal fees from Merck / MSD, personal fees from Berlin Chemie / Menarini, personal fees from Roche Diagnostics, personal fees from Saja Pharmaceuticals, personal fees from Servier, outside the submitted work. DW has nothing to disclose. CBG reports personal fees from Bayer, grants and personal fees from Boehringer Ingelheim, personal fees from Boston Scientific, grants and personal fees from Bristol Myers Squibb, grants from Daiichi Sankyo, grants and personal fees from Janssen, grants and personal fees from Pfizer, during the conduct of the study; personal fees from Abbvie, grants from Akros, grants from AstraZeneca, personal fees from Espero, grants from FDA, grants from Galxo Smith Kline, personal fees from Medscape, personal fees from Medtronic Inc., grants from Medtronic Foundation, personal fees from Merck, personal fees from NIH, personal fees from Novo Nordisk, grants and personal fees from Novartis, personal fees from Roche, grants and personal fees from The Medicine’s Co., grants from Apple, personal fees from Rho Pharmaceuticals, personal fees from CeleCor, personal fees from Correvio, personal fees from Philips, personal fees from Abiomed, personal fees from Anthos Therapeutics, outside the submitted work.
Figures

Comment in
-
A Patient-Level Meta-Analysis: The End of the Era of Direct Oral Anticoagulant Developmental Trials in Patients With Atrial Fibrillation?Circulation. 2022 Jan 25;145(4):256-258. doi: 10.1161/CIRCULATIONAHA.121.058159. Epub 2022 Jan 24. Circulation. 2022. PMID: 35073174 No abstract available.
References
-
- January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC Jr., Ellinor PT, Ezekowitz MD, Field ME, Furie KL, et a 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation 2019;140:e125–e151. - PubMed
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomstrom-Lundqvist C, Boriani G, Castella M, Dan GA, Dilaveris PE, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2021;42:373–498. - PubMed
-
- Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, Pogue J, Reilly PA, Themeles E, Varrone J, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361:1139–1151. - PubMed
-
- Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, Breithardt G, Halperin JL, Hankey GJ, Piccini JP, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011;365:883–891. - PubMed
-
- Granger CB, Alexander JH, McMurray JJ, Lopes RD, Hylek EM, Hanna M, Al-Khalidi HR, Ansell J, Atar D, Avezum A, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2011;365:981–992. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
