

Plasma 5-HIAA activity indicative of serotonergic disturbances in cognitively impaired, elderly patients experiencing postoperative delirium
- PMID: 34985774
- PMCID: PMC9303571
- DOI: 10.1002/gps.5677
Plasma 5-HIAA activity indicative of serotonergic disturbances in cognitively impaired, elderly patients experiencing postoperative delirium
Abstract
Objectives: Delirium frequently arises in older demented and non-demented patients in postoperative, clinical settings. To date, the underlying pathophysiological mechanisms remain poorly understood. Monoamine neurotransmitter alterations have been linked to delirium and cognitive impairment. Our aim was to investigate if this holds true in cognitively normal and impaired patients experiencing delirium following hip surgery.
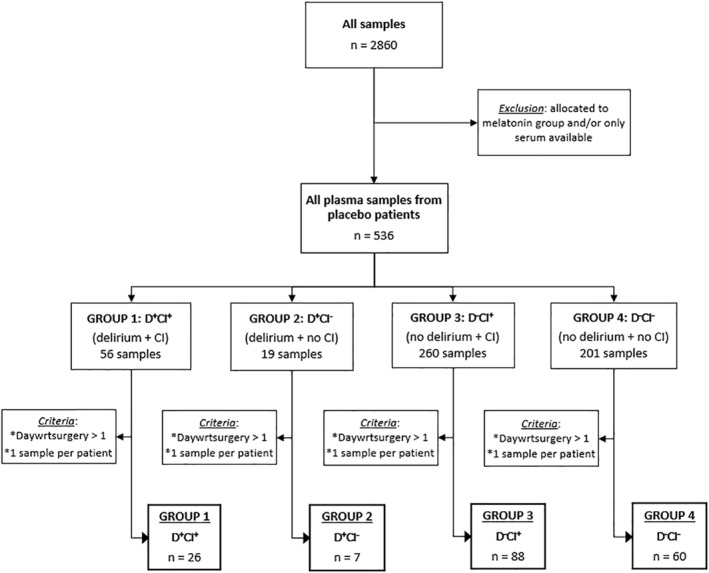
Methods: Monoamines and metabolites were measured in plasma samples of 181 individuals by means of reversed-phase ultra-high-performance liquid chromatography with electrochemical detection. Delirium and delirium severity were scored with the Confusion Assessment Method and Delirium Rating Scale-Revised-1998. Cognitive function was assessed using the Informant Questionnaire on Cognitive Decline and the Mini-Mental State Examination, multimorbidity with the Charlson Comorbidity Index.
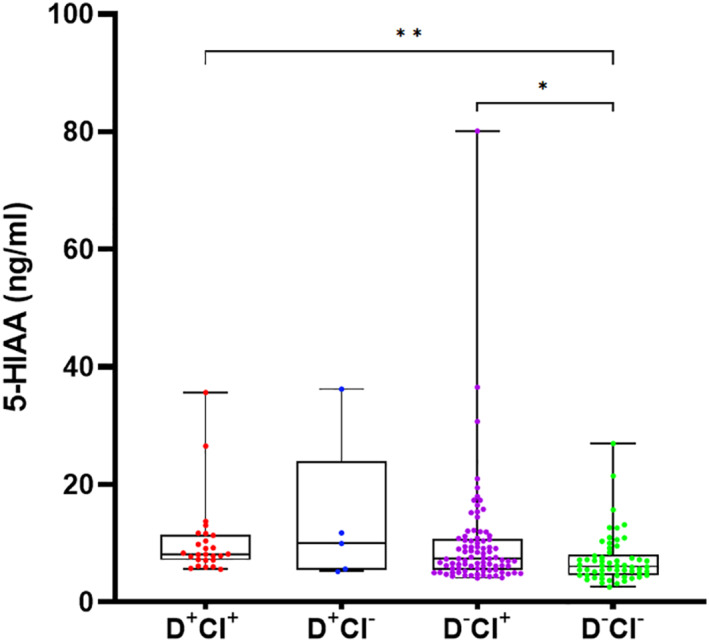
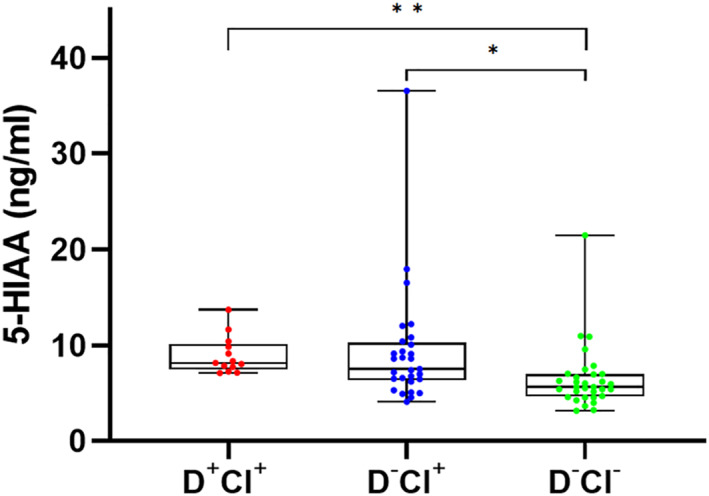
Results: Plasma 5-hydroxyindoleacetic acid (5-HIAA), the major metabolite of serotonin (5-HT), was significantly higher in delirious and non-delirious cognitively impaired subjects as compared to control individuals without delirium and cognitive impairment (p < 0.001 and p = 0.007), which remained highly significant after excluding patients taking psychotropic medication (p < 0.0001 and p = 0.003). No significant differences were found for cognitively normal delirious patients, although serotonergic levels were numerically higher compared to control counterparts.
Conclusions: Our findings indicate a general serotonergic disturbance in delirious and non-delirious postoperative patients suffering from cognitive impairment. We observed a similar, but less pronounced difference in delirious patients, which suggests serotonergic disturbances may be further aggravated by the co-occurrence of delirium and cognitive impairment.
Keywords: HPLC; UPLC; ageing; biogenic amines; biomarker; cognitive impairment; delirium; monoamine neurotransmitters.
© 2021 The Authors. International Journal of Geriatric Psychiatry published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
A long-term follow-up study of cerebrospinal fluid 5-hydroxyindoleacetic acid in delirium.Eur Arch Psychiatry Clin Neurosci. 1994;244(3):131-4. doi: 10.1007/BF02191886. Eur Arch Psychiatry Clin Neurosci. 1994. PMID: 7528542
-
Clinical characteristics and risk factors of delirium in demented and not demented elderly medical inpatients.J Nutr Health Aging. 2006 Nov-Dec;10(6):535-9. J Nutr Health Aging. 2006. PMID: 17183425
-
Abnormal neurotransmitter metabolite levels in Alzheimer patients with a delirium.Int J Geriatr Psychiatry. 2006 Sep;21(9):838-43. doi: 10.1002/gps.1569. Int J Geriatr Psychiatry. 2006. PMID: 16955437
-
[Perioperative disorders of mental functions].Acta Med Croatica. 2012 Mar;66(1):73-9. Acta Med Croatica. 2012. PMID: 23088091 Review. Croatian.
-
Lipid dysregulation and delirium in older adults: A review of the current evidence and future directions.Brain Res Bull. 2025 May;224:111299. doi: 10.1016/j.brainresbull.2025.111299. Epub 2025 Mar 12. Brain Res Bull. 2025. PMID: 40086765 Review.
Cited by
-
Projection of visual material on postoperative delirium in patients undergoing cardiac surgery: A double blind randomized clinical trial.Medicine (Baltimore). 2024 Oct 4;103(40):e39470. doi: 10.1097/MD.0000000000039470. Medicine (Baltimore). 2024. PMID: 39465770 Free PMC article. Clinical Trial.
-
Mechanisms underlying delirium in patients with critical illness.Front Aging Neurosci. 2024 Sep 26;16:1446523. doi: 10.3389/fnagi.2024.1446523. eCollection 2024. Front Aging Neurosci. 2024. PMID: 39391586 Free PMC article. Review.
-
Repetitive transcranial magnetic stimulation elevates the serum levels of neurotrophic factors and serotonin and its metabolites in patients with ischemic stroke.Front Neurol. 2025 Mar 5;16:1513131. doi: 10.3389/fneur.2025.1513131. eCollection 2025. Front Neurol. 2025. PMID: 40109842 Free PMC article.
References
-
- APA . Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
