

Integrative clinical and molecular characterization of translocation renal cell carcinoma
- PMID: 34986355
- PMCID: PMC9127595
- DOI: 10.1016/j.celrep.2021.110190
Integrative clinical and molecular characterization of translocation renal cell carcinoma
Abstract
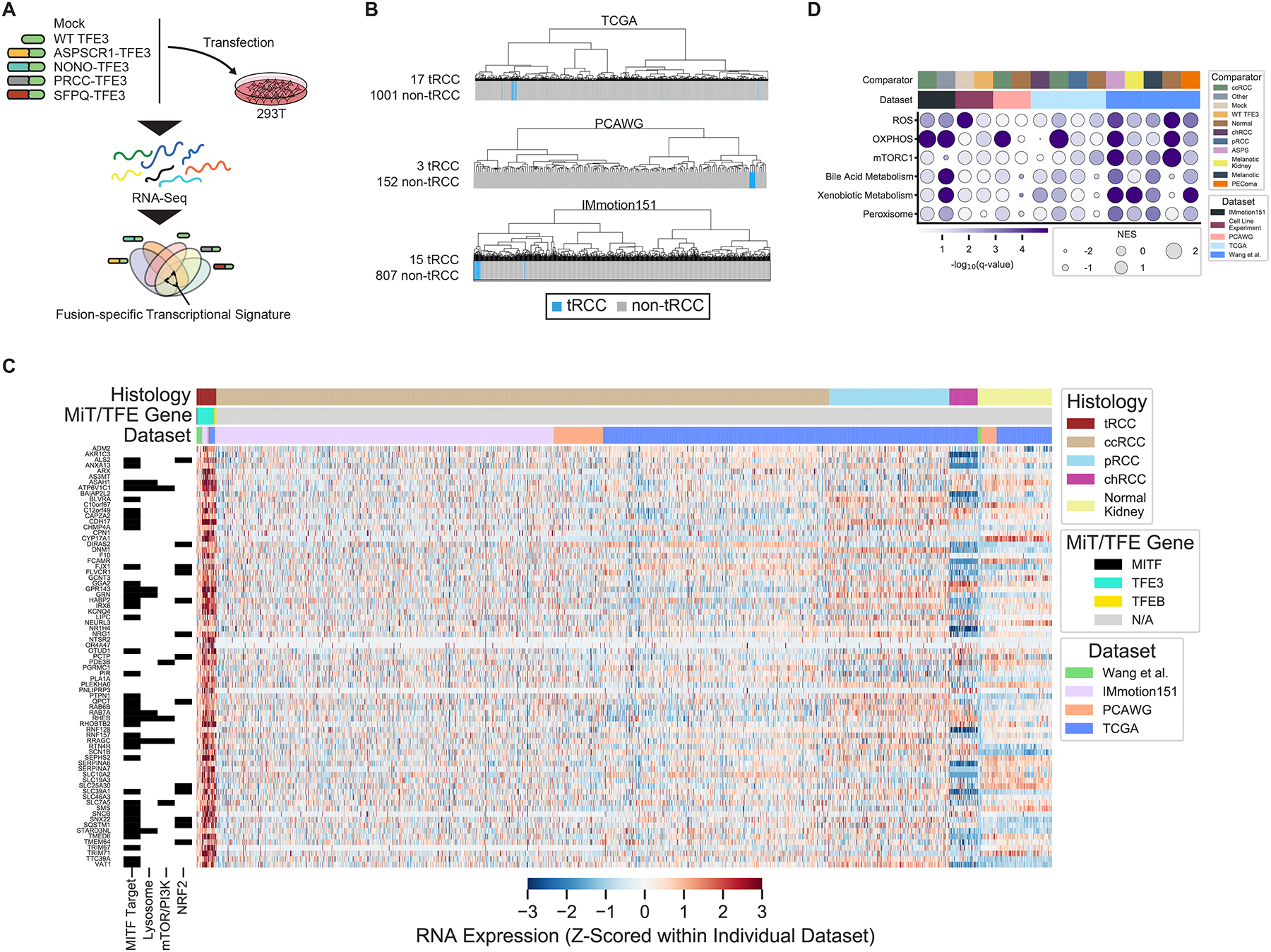
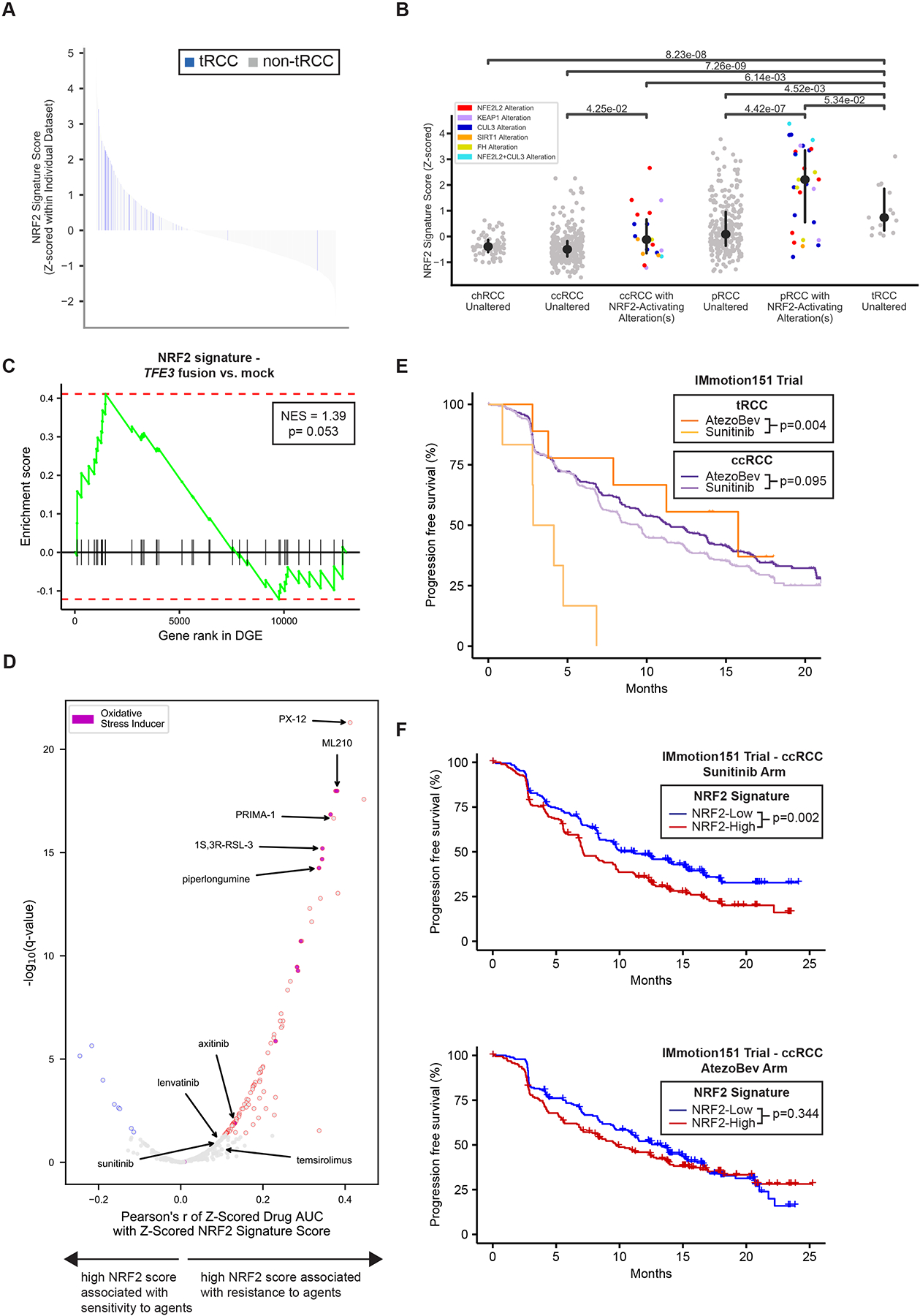
Translocation renal cell carcinoma (tRCC) is a poorly characterized subtype of kidney cancer driven by MiT/TFE gene fusions. Here, we define the landmarks of tRCC through an integrative analysis of 152 patients with tRCC identified across genomic, clinical trial, and retrospective cohorts. Most tRCCs harbor few somatic alterations apart from MiT/TFE fusions and homozygous deletions at chromosome 9p21.3 (19.2% of cases). Transcriptionally, tRCCs display a heightened NRF2-driven antioxidant response that is associated with resistance to targeted therapies. Consistently, we find that outcomes for patients with tRCC treated with vascular endothelial growth factor receptor inhibitors (VEGFR-TKIs) are worse than those treated with immune checkpoint inhibitors (ICI). Using multiparametric immunofluorescence, we find that the tumors are infiltrated with CD8+ T cells, though the T cells harbor an exhaustion immunophenotype distinct from that of clear cell RCC. Our findings comprehensively define the clinical and molecular features of tRCC and may inspire new therapeutic hypotheses.
Keywords: MITF; NRF2; TFE3; TFEB; VEGFR; genomics; immune checkpoint inhibition; immunotherapy; oxidative stress; translocation renal cell carcinoma.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests Z.B.: research funding from Bristol-Myers Squibb & Genentech/imCORE; honoraria from UpToDate. X.G.: advisory board for Exelixis, Bayer and Guardant Health. D.A.B.: non-financial support from Bristol Myers Squibb, honoraria from LM Education/Exchange Services, advisory board fees from Exelixis and Aveo, and consulting/personal fees from Octane Global, Defined Health, Dedham Group, Adept Field Solutions, Slingshot Insights, Blueprint Partnerships, Charles River Associates, Trinity Group, and Insight Strategy outside of the submitted work. N.I.V.: advisory board to Sanofi/Genzyme, Oncocyte, and Lilly. M.S.H.: consultant, Janssen Pharmaceuticals and UpToDate. R.H.: research funding from Novartis. B.A.M.: consultant for Bayer, Astellas, AstraZeneca, Seattle Genetics, Exelixis, Nektar, Pfizer, Janssen, Genentech, Eisai, Dendreon, Bristol Myers Squibb, Calithera, and EMD Serono; research funding to the institution from Bristol Myers Squibb, Calithera, Exelixis, and Seattle Genetics. A.S.F.: consultant, Olympus America, Inc.; honoraria, Roche, Janssen; advisory board, Vessi Medical. C.J.W.: equity holder of BioNTech, Inc; research funding from Pharmacyclics. D.F.M.: honoraria from BMS, Pfizer, Merck, Alkermes, Inc., EMD Serono, Eli Lilly and Company, Iovance, Eisai, Inc., Werewolf Therapeutics, and Calithera Biosciences; research support from BMS, Merck, Genentech, Pfizer, Exelixis, X4 Pharma, and Alkermes, Inc. D.Y.C.H.: consultancies and research funding from Pfizer, Novartis, BMS, Merck, Eisai, Ipsen, and Exelixis. S.S.: grants from Exelixis, grants from Bristol-Myers Squibb, personal fees from Merck, grants and personal fees from AstraZeneca, personal fees from CRISPR Therapeutics, personal fees from NCI, and personal fees from AACR; a patent for Biogenex with royalties paid. E.M.V.A.: advisory/consulting, Tango Therapeutics, Genome Medical, Invitae, Enara Bio, Janssen, Manifold Bio, Monte Rosa; research support, Novartis, BMS; equity, Tango Therapeutics, Genome Medical, Syapse, Enara Bio, Manifold Bio, Microsoft, Monte Rosa; patents, institutional patents filed on chromatin mutations and immunotherapy response and methods for clinical interpretation. T.K.C.: research (institutional and personal), Alexion, Analysis Group, AstraZeneca, Aveo, Bayer, Bristol Myers-Squibb/ER Squibb and Sons, LLC, Calithera, Cerulean, Corvus, Eisai, Exelixis, F. Hoffmann-La Roche, Foundation Medicine, Inc., Genentech, GlaxoSmithKline, Ipsen, Lilly, Merck, Novartis, Peloton, Pfizer, Prometheus Labs, Roche, Roche Products Limited, Sanofi/Aventis, Takeda, and Tracon; consulting/honoraria or advisory role, Alexion, Analysis Group, AstraZeneca, Aveo, Bayer, Bristol Myers-Squibb/ER Squibb and Sons, LLC, Cerulean, Corvus, Eisai, EMD Serono, Exelixis, Foundation Medicine, Inc., Genentech, GlaxoSmithKline, Heron Therapeutics, Infinity Pharma, Ipsen, Jansen Oncology, IQVIA, Lilly, Merck, NCCN, Novartis, Nuscan, Peloton, Pfizer, Pionyr, Prometheus Labs, Roche, Sanofi/Aventis, Surface Oncology, Tempest, and Up-to-Date; CME-related events (e.g., OncLIve, PVI, MJH Life Sciences); NCI GU Steering Committee; stock ownership, Pionyr and Tempest; patents filed, royalties, or other intellectual properties, related to biomarkers of immune checkpoint blockers and ctDNA; travel, accommodations, expenses, medical writing in relation to consulting, advisory roles, or honoraria; no speaker’s bureau. S.R.V.: consulting, MPM Capital and Vida Ventures; spouse is an employee of and holds equity in Kojin Therapeutics. All other authors report no competing interests.
Figures




References
-
- Adam J, Hatipoglu E, O’Flaherty L, Ternette N, Sahgal N, Lockstone H, Baban D, Nye E, Stamp GW, Wolhuter K, et al. (2011). Renal Cyst Formation in Fh1-Deficient Mice Is Independent of the Hif/Phd Pathway: Roles for Fumarate in KEAP1 Succination and Nrf2 Signaling. Cancer Cell 20, 524–537. - PMC - PubMed
-
- Álvarez-Fernández M, and Malumbres M (2020). Mechanisms of Sensitivity and Resistance to CDK4/6 Inhibition. Cancer Cell 37, 514–529. - PubMed
-
- Ambalavanan M, and Geller JI (2019). Treatment of advanced pediatric renal cell carcinoma. Pediatr Blood Cancer 66, e27766. - PubMed
-
- Argani P, Olgac S, Tickoo SK, Goldfischer M, Moch H, Chan DY, Eble JN, Bonsib SM, Jimeno M, Lloreta J, et al. (2007). Xp11 Translocation Renal Cell Carcinoma in Adults: Expanded Clinical, Pathologic, and Genetic Spectrum. The American Journal of Surgical Pathology 31, 1149–1160. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
