

Treatment patterns and survival in advanced unresectable esophageal squamous cell cancer: A population-based study
- PMID: 34986523
- PMCID: PMC8898723
- DOI: 10.1111/cas.15262
Treatment patterns and survival in advanced unresectable esophageal squamous cell cancer: A population-based study
Abstract
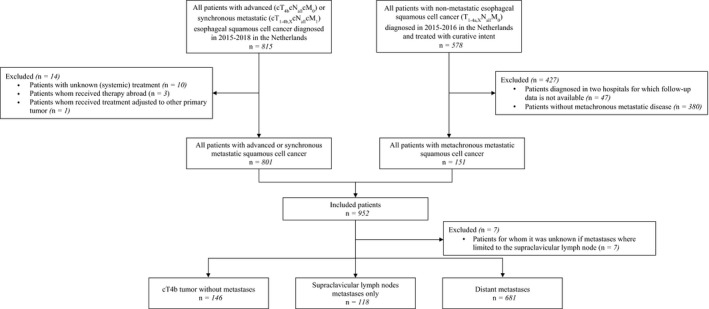
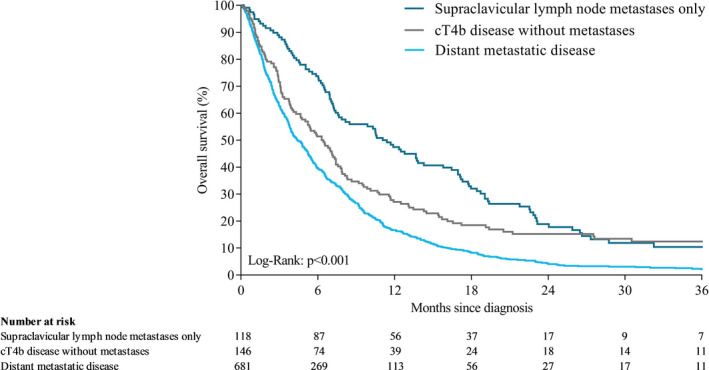
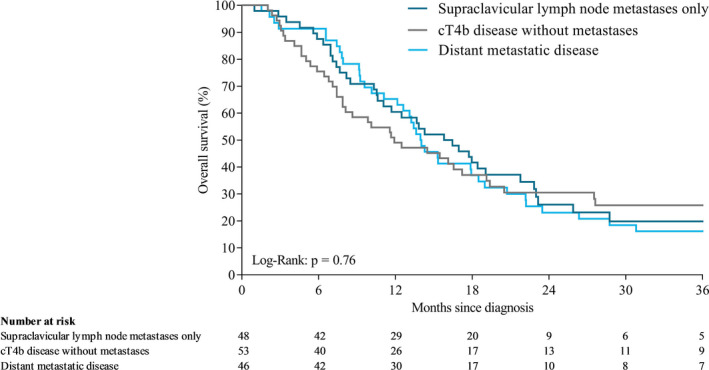
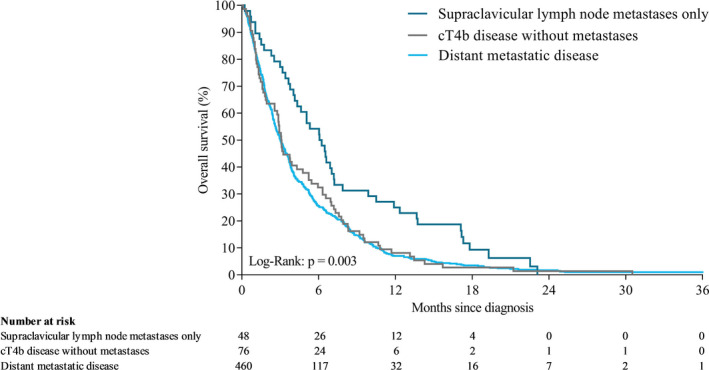
Data on treatment and survival of patients with advanced unresectable esophageal squamous cell carcinoma (ESCC) from Western populations are limited. Here we describe treatment and survival in patients with advanced unresectable ESCC: patients with cT4b disease without metastases (cT4b), metastases limited to the supraclavicular lymph nodes (SCLNM) or distant metastatic ESCC at the population level. All patients with unresectable (cT4b) or synchronous metastatic ESCC at primary diagnosis (2015-2018) or patients with metachronous metastases after primary non-metastatic diagnosis in 2015-2016 were selected from the Netherlands Cancer Registry. Fifteen percent of patients had cT4b disease (n = 146), 12% SCLNM (n = 118) and 72% distant metastases (n = 681). Median overall survival (OS) time was 6.3, 11.2, and 4.4 months in patients with cT4b, SCLNM, and distant metastases, respectively (P < .001). Multivariable Cox regression showed that patients with cT4b (hazard ratio 1.44, 95% CI 1.04-1.99) and patients with distant metastases (hazard ratio 1.42, 95% CI 1.12-1.80) had a worse survival time compared with patients with SCLNM. Among patients who received chemoradiotherapy and/or underwent resection (primary tumor and/or metastases), median OS was 11.9, 16.1, and 14.0 months in patients with cT4b, SCLNM, and distant metastases, respectively (P = .76). Patients with SCLNM had a better survival time compared with patients with cT4b and patients with distant metastases. Survival of patients with advanced unresectable ESCC in clinical practice was poor, even in patients treated with curative intent.
Keywords: distant metastases; esophageal squamous cell carcinoma; palliative treatment; supraclavicular lymph node metastases; unresectable advanced disease.
© 2022 The Authors. Cancer Science published by John Wiley & Sons Australia, Ltd on behalf of Japanese Cancer Association.
Conflict of interest statement
JdV has served as a consultant for Amgen, AstraZeneca, MSD, Pierre Fabre, and Servier, and has received institutional research funding from Servier. HvL reports grants from Roche, has served as a consultant for BMS, Celgene, Lilly, and Nordic and has received unrestricted research funding from Bayer, BMS, Celgene, Lilly, Merck Serono, MSD, Nordic, Philips, and Roche. RV reports grants from BMS and Roche. MP, PV, MH, SG, and PJ have no disclosures to declare.
Figures
References
-
- Arnold M, Soerjomataram I, Ferlay J, Forman D. Global incidence of oesophageal cancer by histological subtype in 2012. Gut. 2015;64:381‐387. - PubMed
-
- Ter Veer E, Haj Mohammad N, van Valkenhoef G, et al. The efficacy and safety of first‐line chemotherapy in advanced esophagogastric cancer: a network meta‐analysis. J Natl Cancer Inst. 2016;108:djw166. - PubMed
-
- van Kleef JJ, Ter Veer E, van den Boorn HG, et al. Quality of life during palliative systemic therapy for esophagogastric cancer: systematic review and meta‐analysis. J Natl Cancer Inst. 2020;112:12‐29. - PubMed
-
- TNM . Classification of Malignant Tumours, 8th edn: Wiley‐Blackwell, International Union Against Cancer (UICC); 2017.
-
- Jeene PM, Versteijne E, van Berge Henegouwen MI, et al. Supraclavicular node disease is not an independent prognostic factor for survival of esophageal cancer patients treated with definitive chemoradiation. Acta Oncol. 2017;56:33‐38. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
