

Evidence-based cardiovascular magnetic resonance cost-effectiveness calculator for the detection of significant coronary artery disease
- PMID: 34986851
- PMCID: PMC8734365
- DOI: 10.1186/s12968-021-00833-1
Evidence-based cardiovascular magnetic resonance cost-effectiveness calculator for the detection of significant coronary artery disease
Erratum in
-
Correction to: J Cardiovasc Magn Reson, volume 24.J Cardiovasc Magn Reson. 2022 Mar 16;24(1):17. doi: 10.1186/s12968-022-00847-3. J Cardiovasc Magn Reson. 2022. PMID: 35296337 Free PMC article. No abstract available.
Abstract
Background: Although prior reports have evaluated the clinical and cost impacts of cardiovascular magnetic resonance (CMR) for low-to-intermediate-risk patients with suspected significant coronary artery disease (CAD), the cost-effectiveness of CMR compared to relevant comparators remains poorly understood. We aimed to summarize the cost-effectiveness literature on CMR for CAD and create a cost-effectiveness calculator, useable worldwide, to approximate the cost-per-quality-adjusted-life-year (QALY) of CMR and relevant comparators with context-specific patient-level and system-level inputs.
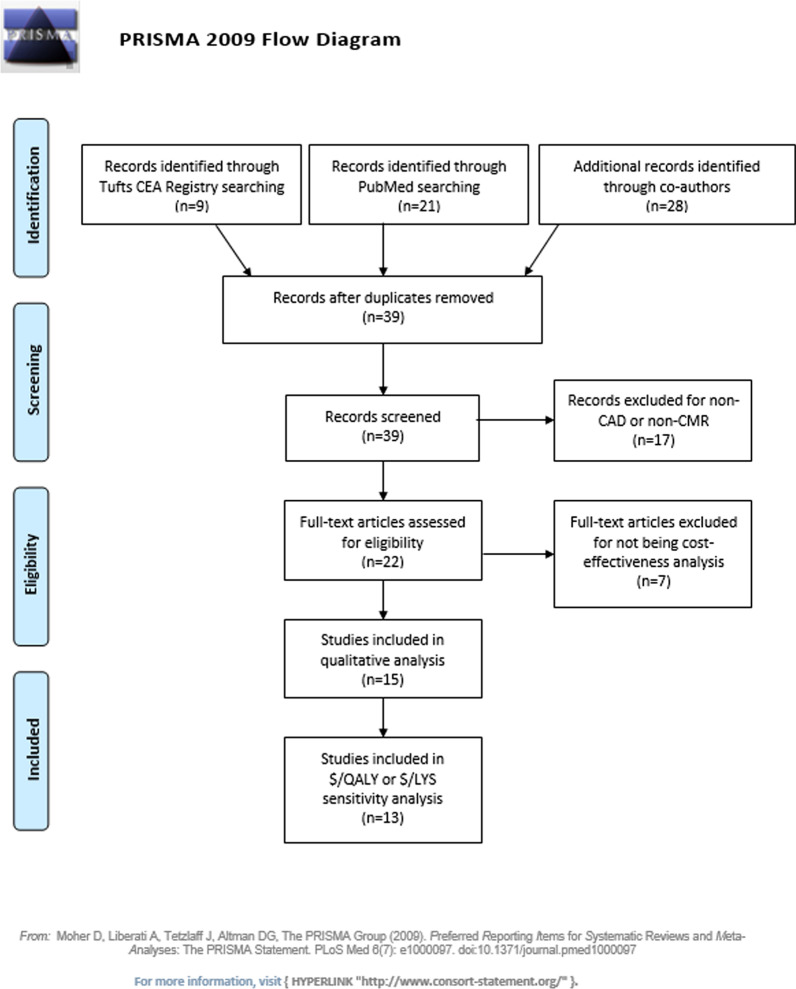
Methods: We searched the Tufts Cost-Effectiveness Analysis Registry and PubMed for cost-per-QALY or cost-per-life-year-saved studies of CMR to detect significant CAD. We also developed a linear regression meta-model (CMR Cost-Effectiveness Calculator) based on a larger CMR cost-effectiveness simulation model that can approximate CMR lifetime discount cost, QALY, and cost effectiveness compared to relevant comparators [such as single-photon emission computed tomography (SPECT), coronary computed tomography angiography (CCTA)] or invasive coronary angiography.
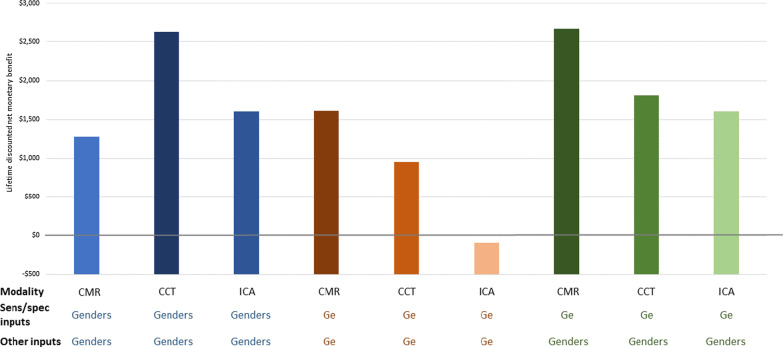
Results: CMR was cost-effective for evaluation of significant CAD (either health-improving and cost saving or having a cost-per-QALY or cost-per-life-year result lower than the cost-effectiveness threshold) versus its relevant comparator in 10 out of 15 studies, with 3 studies reporting uncertain cost effectiveness, and 2 studies showing CCTA was optimal. Our cost-effectiveness calculator showed that CCTA was not cost-effective in the US compared to CMR when the most recent publications on imaging performance were included in the model.
Conclusions: Based on current world-wide evidence in the literature, CMR usually represents a cost-effective option compared to relevant comparators to assess for significant CAD.
Keywords: Cardiovascular magnetic resonance; Coronary artery disease; Cost-effectiveness.
© 2021. The Author(s).
Conflict of interest statement
S. Kelle receives research funding by Novartis and Philips Healthcare. S. E. Petersen provides consultancy to and is a shareholder of Circle Cardiovascular Imaging Inc, Calgary, Canada. J. Schwitter and E. Nagel receive research funding by Bayer Healthcare. J. White is a shareholder of Cohesic Inc. S. Kelle and E. Nagel are supported by the DZHK (German Centre for Cardiovascular Research) and by the BMBF (German Ministry of Education and Research). CBD is the Chief Executive Officer (part time) of the Society for Cardiovascular Magnetic Resonance (SCMR). JC was president of the Society for Cardiovascular Magnetic Resonance (SCMR) at the time this work was performed, receives research support from Bayer, Siemens, Guerbet, advisory board/lectures for Bayer, Siemens, Bracco. The other co-authors have no disclosures.
Figures

References
-
- Mark DB, Anderson JL, Brinker JA, Brophy JA, Casey DE, Jr, Cross RR, Edmundowicz D, Hachamovitch R, Hlatky MA, Jacobs JE, Jaskie S, Kett KG, Malhotra V, Masoudi FA, McConnell MV, Rubin GD, Shaw LJ, Sherman ME, Stanko S, Ward RP. ACC/AHA/ASE/ASNC/HRS/IAC/Mended Hearts/NASCI/RSNA/SAIP/SCAI/SCCT/SCMR/SNMMI 2014 health policy statement on use of noninvasive cardiovascular imaging: a report of the American College of Cardiology Clinical Quality Committee. J Am Coll Cardiol. 2014;63:698–721. doi: 10.1016/j.jacc.2013.02.002. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
