

Body composition, physical capacity, and immuno-metabolic profile in community-acquired pneumonia caused by COVID-19, influenza, and bacteria: a prospective cohort study
- PMID: 34987205
- PMCID: PMC8729099
- DOI: 10.1038/s41366-021-01057-0
Body composition, physical capacity, and immuno-metabolic profile in community-acquired pneumonia caused by COVID-19, influenza, and bacteria: a prospective cohort study
Abstract
Background: Different pathogens can cause community-acquired pneumonia (CAP); however, the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causing coronavirus disease 2019 (COVID-19) has re-emphasized the vital role of respiratory viruses as a cause of CAP. The aim was to explore differences in metabolic profile, body composition, physical capacity, and inflammation between patients hospitalized with CAP caused by different etiology.
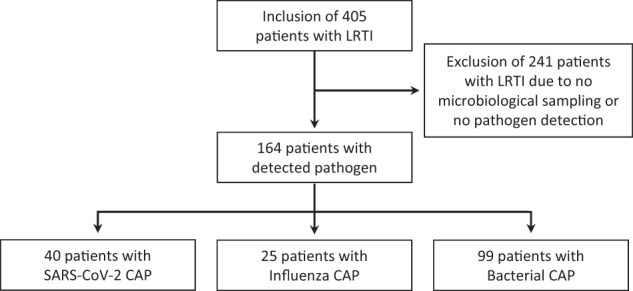
Methods: A prospective study of Danish patients hospitalized with CAP caused by SARS-CoV-2, influenza, or bacteria. Fat (FM) and fat-free mass (FFM) were assessed with bioelectrical impedance analysis. Physical activity and capacity were assessed using questionnaires and handgrip strength. Plasma (p)-glucose, p-lipids, hemoglobin A1c (HbA1c), p-adiponectin, and cytokines were measured.
Results: Among 164 patients with CAP, etiology did not affect admission levels of glucose, HbA1c, adiponectin, or lipids. Overall, 15.2% had known diabetes, 6.1% had undiagnosed diabetes, 51.3% had pre-diabetes, 81% had hyperglycemia, and 60% had low HDL-cholesterol, with no difference between groups. Body mass index, FM, and FFM were similar between groups, with 73% of the patients being characterized with abdominal obesity, although waist circumference was lower in patients with COVID-19. Physical capacity was similar between groups. More than 80% had low handgrip strength and low physical activity levels. Compared to patients with influenza, patients with COVID-19 had increased levels of interferon (IFN)-γ (mean difference (MD) 4.14; 95% CI 1.36-12.58; p = 0.008), interleukin (IL)-4 (MD 1.82; 95% CI 1.12-2.97; p = 0.012), IL-5 (MD 2.22; 95% CI 1.09-4.52; p = 0.024), and IL-6 (MD 2.41; 95% CI 1.02-5.68; p = 0.044) and increased IFN-γ (MD 6.10; 95% CI 2.53-14.71; p < 0.001) and IL-10 (MD 2.68; 95% CI 1.53-4.69; p < 0.001) compared to patients with bacterial CAP, but no difference in IL-1β, tumor necrosis factor-α, IL-8, IL-18, IL-12p70, C-reactive protein, and adiponectin.
Conclusion: Despite higher inflammatory response in patients with COVID-19, metabolic profile, body composition, and physical capacity were similar to patients with influenza and bacterial CAP.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Piroth L, Cottenet J, Mariet A-S, Bonniaud P, Blot M, Tubert-Bitter P, et al. Comparison of the characteristics, morbidity, and mortality of COVID-19 and seasonal influenza: a nationwide, population-based retrospective cohort study. Lancet Respir Med. 2021;9:251–9. doi: 10.1016/S2213-2600(20)30527-0. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
