

Informed decision-making in delivery of dialysis: combining clinical outcomes with sustainability
- PMID: 34987789
- PMCID: PMC8711764
- DOI: 10.1093/ckj/sfab193
Informed decision-making in delivery of dialysis: combining clinical outcomes with sustainability
Abstract
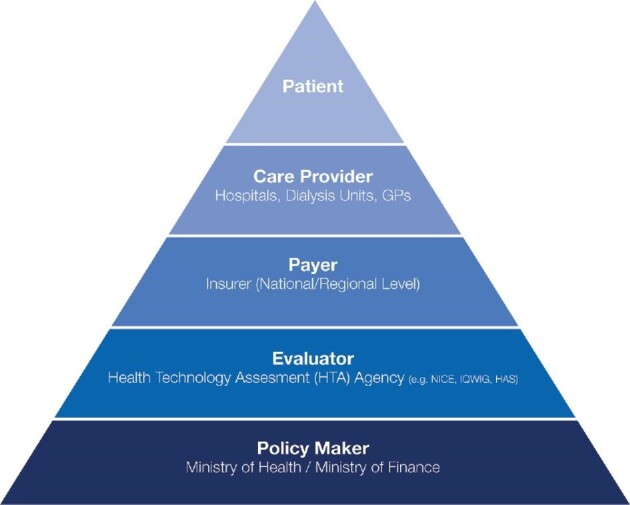
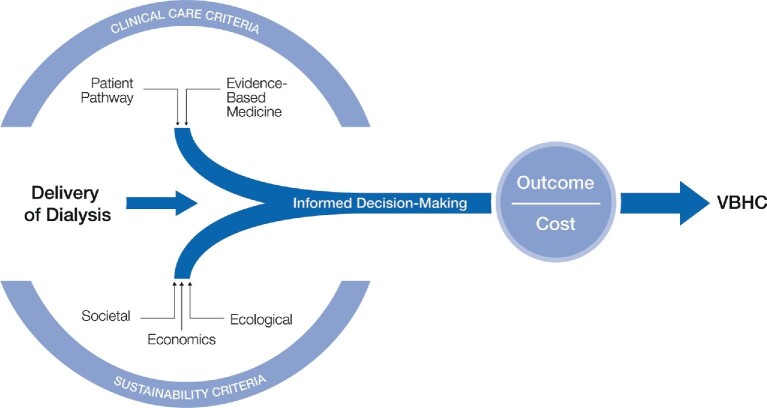
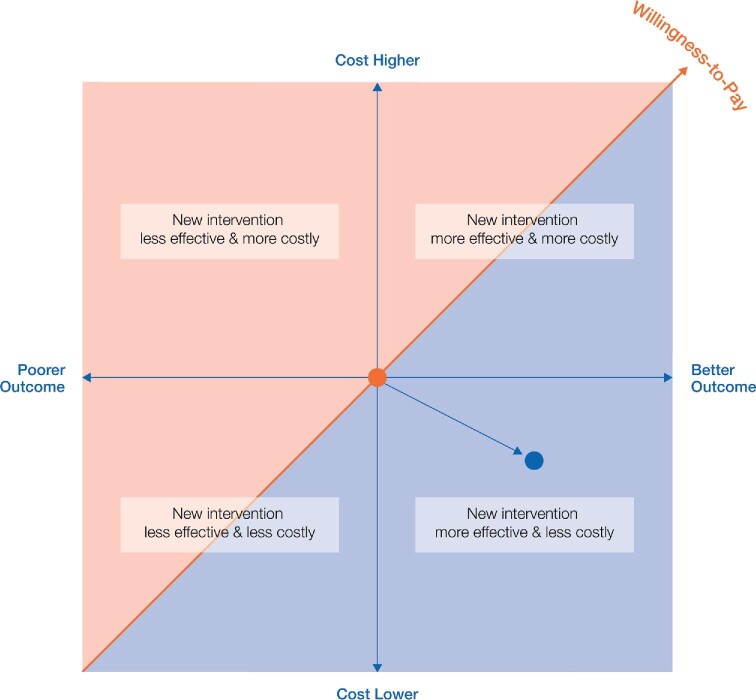
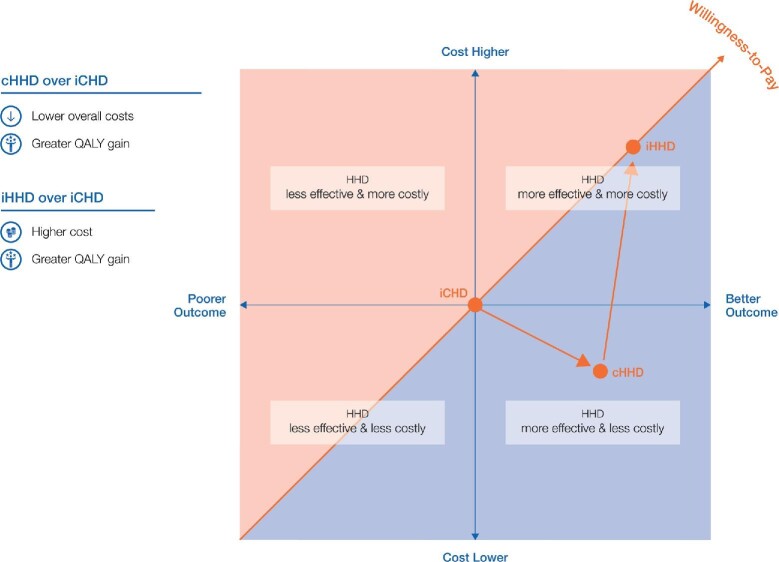
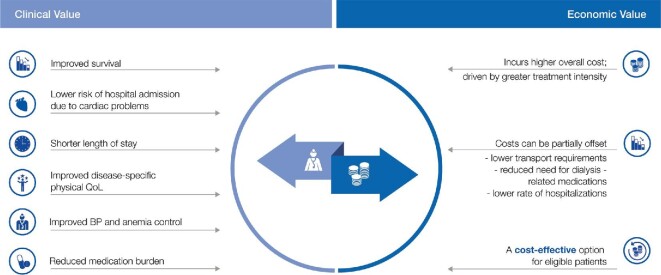
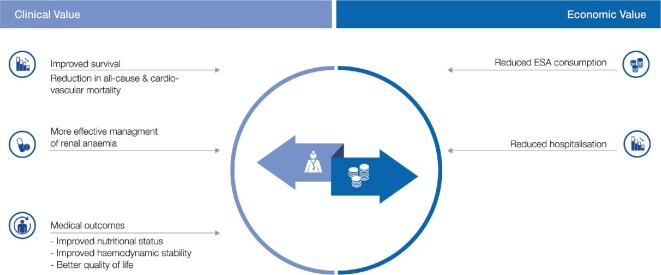
As the prevalence of chronic kidney disease is expected to rise worldwide over the next decades, provision of renal replacement therapy (RRT), will further challenge budgets of all healthcare systems. Most patients today requiring RRT are treated with haemodialysis (HD) therapy and are elderly. This article demonstrates the interdependence of clinical and sustainability criteria that need to be considered to prepare for the future challenges of delivering dialysis to all patients in need. Newer, more sustainable models of high-value care need to be devised, whereby delivery of dialysis is based on value-based healthcare (VBHC) principles, i.e. improving patient outcomes while restricting costs. Essentially, this entails maximizing patient outcomes per amount of money spent or available. To bring such a meaningful change, revised strategies having the involvement of multiple stakeholders (i.e. patients, providers, payers and policymakers) need to be adopted. Although each stakeholder has a vested interest in the value agenda often with conflicting expectations and motivations (or motives) between each other, progress is only achieved if the multiple blocs of the delivery system are advanced as mutually reinforcing entities. Clinical considerations of delivery of dialysis need to be based on the entire patient disease pathway and evidence-based medicine, while the non-clinical sustainability criteria entail, in addition to economics, the societal and ecological implications of HD therapy. We discuss how selection of appropriate modes and features of delivery of HD (e.g. treatment modalities and schedules, selection of consumables, product life cycle assessment) could positively impact decision-making towards value-based renal care. Although the delivery of HD therapy is multifactorial and complex, applying cost-effectiveness analyses for the different HD modalities (conventional in-centre and home HD) can support in guiding payability (balance between clinical value and costs) for health systems. For a resource intensive therapy like HD, concerted and fully integrated care strategies need to be urgently implemented to cope with the global demand and burden of HD therapy.
Keywords: haemodialysis; informed-decision making; sustainability; value-based healthcare.
© The Author(s) 2021. Published by Oxford University Press on behalf of ERA.
Figures
References
-
- Coresh J, Jafar TH. Disparities in worldwide treatment of kidney failure. Lancet 2015; 385: 1926–1928 - PubMed
-
- Liyanage T, Ninomiya T, Jha V et al. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet 2015; 385: 1975–1982 - PubMed
-
- Wongrakpanich S, Susantitaphong P, Isaranuwatchai S et al. Dialysis therapy and conservative management of advanced chronic kidney disease in the elderly: a systematic review. Nephron 2017; 137: 178–189 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
