

Comparison of popliteal artery aneurysm outcomes after open repair and endovascular repair: reducing post-operative type II endoleak and sac enlargement
- PMID: 34988197
- PMCID: PMC8667160
- DOI: 10.21037/atm-21-5631
Comparison of popliteal artery aneurysm outcomes after open repair and endovascular repair: reducing post-operative type II endoleak and sac enlargement
Abstract
Background: This cohort study aimed to evaluate the short- and long-term outcomes of open repair (OR) and endovascular repair (ER) and identify the most suitable graft and approach for treating popliteal artery aneurysm (PAA) patients.
Methods: The data of PAA patients from January 2000 to August 2020 were retrospectively collected and analyzed. The primary endpoints were 30-day mortality, peri-operative complication morbidity, post-operative type II endoleak, and sac- enlargement. The secondary endpoints were primary graft patency, secondary graft patency, the reintervention rate, and overall mortality.
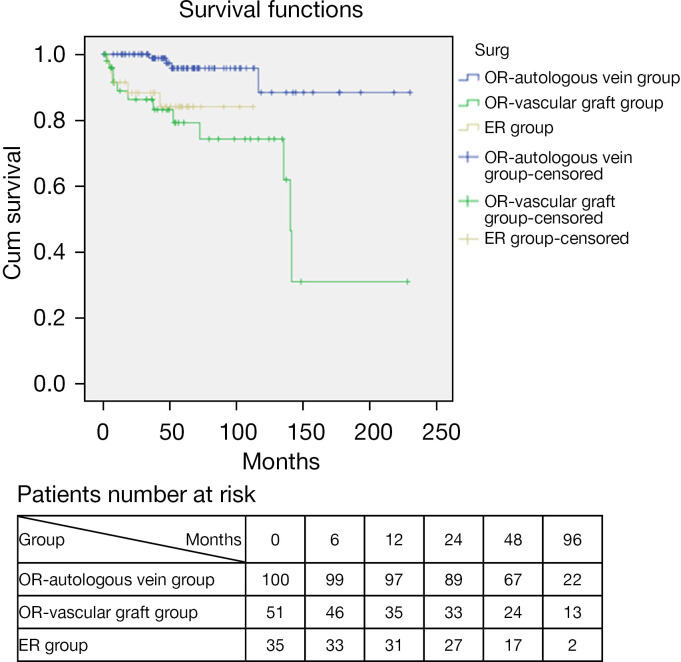
Results: A total of 213 PAAs of 186 patients were surgically repaired. The ER group had a significantly lower mean length of hospital stay, blood loss volume, and aneurysm diameter than the OR group. There were no significant differences between the ER and OR groups in terms of average surgery time, 30-day mortality, peri-operative complication morbidity, post-operative type II endoleak, sac enlargement, primary and secondary graft patency, reintervention rate, and overall mortality. However, in the sub-group analysis, autologous vein grafts had significantly higher primary and secondary graft patency rates than expanded polytetrafluoroethylene (ePTFE) vascular grafts and stent grafts. Type II endoleaks and post-operative sac enlargements were less likely to occur in OR patients when the posterior approach was adopted.
Conclusions: We failed to establish any difference in superiority between OR or ER. However, we found that autologous vein grafts have better graft patency and the posterior approach is less likely to lead to type II endoleaks and sac enlargements after the initial PAA surgical procedure. However, more high-quality, large-scale randomized controlled trials need to be conducted.
Keywords: Popliteal artery aneurysm (PAA); endovascular repair (ER); open repair (OR); procedure approach; type II endoleak.
2021 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://dx.doi.org/10.21037/atm-21-5631). The authors have no conflicts of interest to declare.
Figures





References
LinkOut - more resources
Full Text Sources