

On the Treatment of Pneumocystis jirovecii Pneumonia: Current Practice Based on Outdated Evidence
- PMID: 34988242
- PMCID: PMC8694206
- DOI: 10.1093/ofid/ofab545
On the Treatment of Pneumocystis jirovecii Pneumonia: Current Practice Based on Outdated Evidence
Abstract
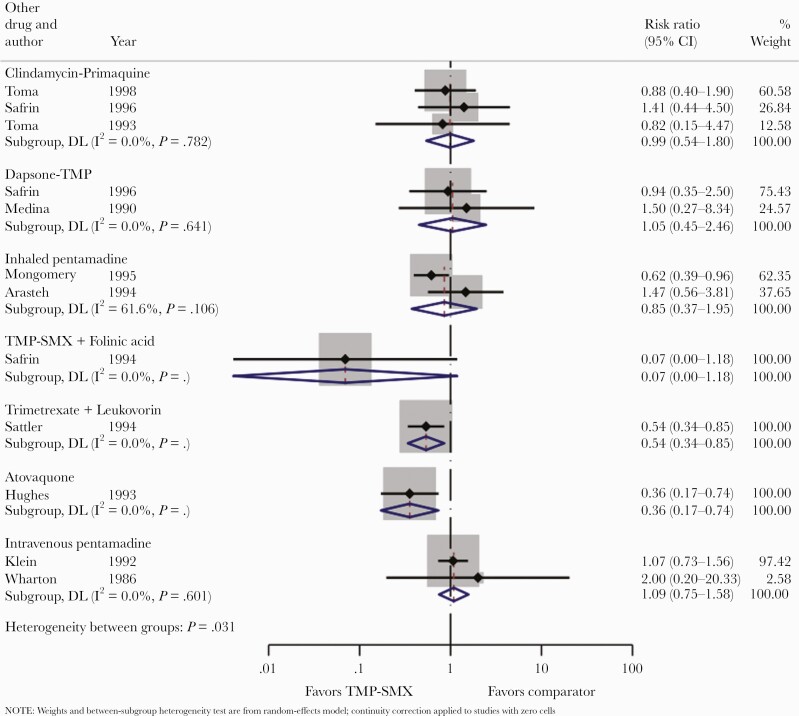
Pneumocystis jirovecii pneumonia (PCP) is a common opportunistic infection causing more than 400000 cases annually worldwide. Although antiretroviral therapy has reduced the burden of PCP in persons with human immunodeficiency virus (HIV), an increasing proportion of cases occur in other immunocompromised populations. In this review, we synthesize the available randomized controlled trial (RCT) evidence base for PCP treatment. We identified 14 RCTs that were conducted 25-35 years ago, principally in 40-year-old men with HIV. Trimethoprim-sulfamethoxazole, at a dose of 15-20 mg/kg per day, is the treatment of choice based on historical practice rather than on quality comparative, dose-finding studies. Treatment duration is similarly based on historical practice and is not evidence based. Corticosteroids have a demonstrated role in hypoxemic patients with HIV but have yet to be studied in RCTs as an adjunctive therapy in non-HIV populations. The echinocandins are potential synergistic treatments in need of further investigation.
Keywords: HIV; Pneumocystis jirovecii pneumonia; TMP-SMX; immunosuppressed; opportunistic infectious.
© The Author(s) 2021. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures



References
-
- Ponce CA, Gallo M, Bustamante R, Vargas SL.. Pneumocystis colonization is highly prevalent in the autopsied lungs of the general population. Clin Infect Dis 2010; 50:347–53. - PubMed
