

Use of biomaterials in corneal endothelial repair
- PMID: 34988369
- PMCID: PMC8721373
- DOI: 10.1177/25158414211058249
Use of biomaterials in corneal endothelial repair
Abstract
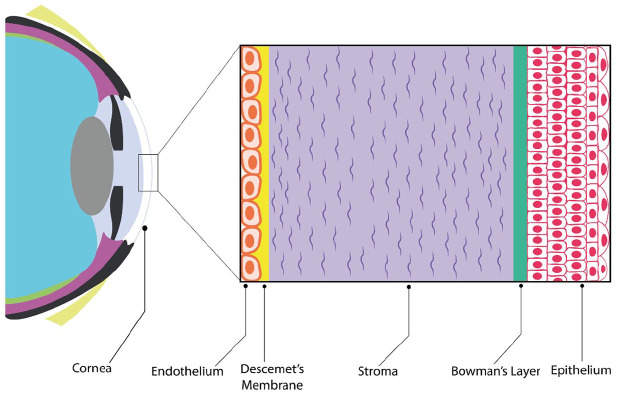
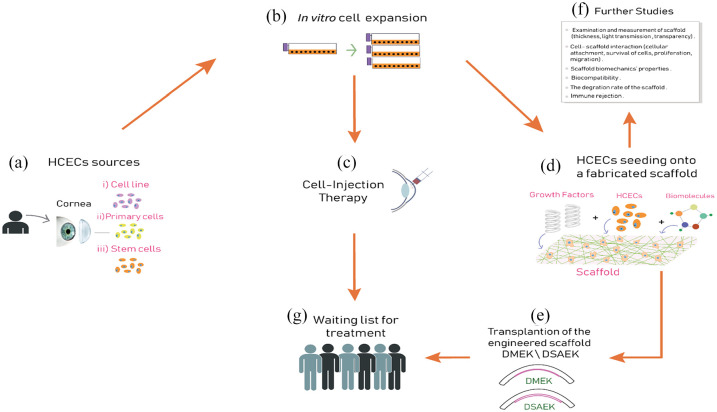
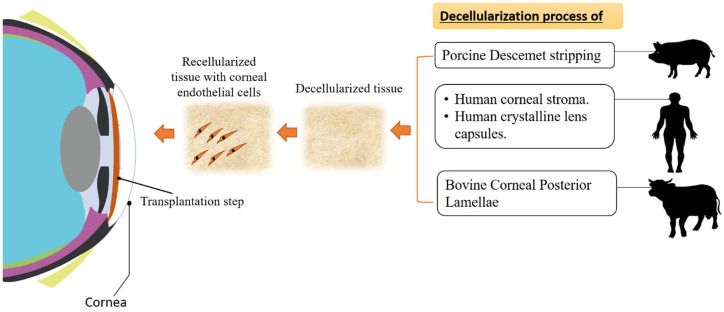
Human corneal endothelium (HCE) is a single layer of hexagonal cells that lines the posterior surface of the cornea. It forms the barrier that separates the aqueous humor from the rest of the corneal layers (stroma and epithelium layer). This layer plays a fundamental role in maintaining the hydration and transparency of the cornea, which in turn ensures a clear vision. In vivo, human corneal endothelial cells (HCECs) are generally believed to be nonproliferating. In many cases, due to their nonproliferative nature, any damage to these cells can lead to further issues with Descemet's membrane (DM), stroma and epithelium which may ultimately lead to hazy vision and blindness. Endothelial keratoplasties such as Descemet's stripping automated endothelial keratoplasty (DSAEK) and Descemet's membrane endothelial keratoplasty (DEK) are the standard surgeries routinely used to restore vision following endothelial failure. Basically, these two similar surgical techniques involve the replacement of the diseased endothelial layer in the center of the cornea by a healthy layer taken from a donor cornea. Globally, eye banks are facing an increased demand to provide corneas that have suitable features for transplantation. Consequently, it can be stated that there is a significant shortage of corneal grafting tissue; for every 70 corneas required, only 1 is available. Nowadays, eye banks face long waiting lists due to shortage of donors, seriously aggravated when compared with previous years, due to the global COVID-19 pandemic. Thus, there is an urgent need to find alternative and more sustainable sources for treating endothelial diseases, such as utilizing bioengineering to use of biomaterials as a remedy. The current review focuses on the use of biomaterials to repair the corneal endothelium. A range of biomaterials have been considered based on their promising results and outstanding features, including previous studies and their key findings in the context of each biomaterial.
Keywords: Descemet’s membrane (DM); biomaterials; cornea; corneal transplantation; human corneal endothelial cells (HCECs); scaffold; tissue engineering.
© The Author(s), 2021.
Conflict of interest statement
Conflict of interest statement: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures


References
-
- Jirsova K. The cornea, anatomy and function no title. In: Jirsova K. (ed.) Light and specular microscopy of the cornea. Cham: Springer, 2017, pp. 1–21.
-
- Nishida T, Saika S, Morishige N. Cornea and sclera: anatomy and physiology. In: Mannis MJ, Holland EJ. (eds) Cornea: fundamentals, diagnosis and management. New York: Elsevier, 2010, pp. 1–22.
-
- Bahn CF, Falls HF, Varley GA, et al.. Classification of corneal endothelial disorders based on neural crest origin. Ophthalmology 1984; 91: 558–563. - PubMed
-
- Soh YQ, Peh G, George BL, et al.. Predicative factors for corneal endothelial cell migration. Invest Ophthalmol Vis Sci 2016; 57: 338–348. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
