

Improving Medication Access within Integrated Treatment for Individuals with Co-Occurring Disorders in Substance Use Treatment Agencies
- PMID: 34988462
- PMCID: PMC8726008
- DOI: 10.1177/26334895211033659
Improving Medication Access within Integrated Treatment for Individuals with Co-Occurring Disorders in Substance Use Treatment Agencies
Abstract
Background: The best approach to provide comprehensive care for individuals with co-occurring disorders (CODs) related to substance use and mental health is to address both disorders through an integrated treatment approach. However, only 25% of behavioral health agencies offer integrated care and less than 7% of individuals who need integrated treatment receive it. A project used a cluster-randomized waitlist control group design to evaluate the effectiveness of Network for the Improvement of Addiction Treatment (NIATx) implementation strategies to improve access to addiction and psychotropic medications.
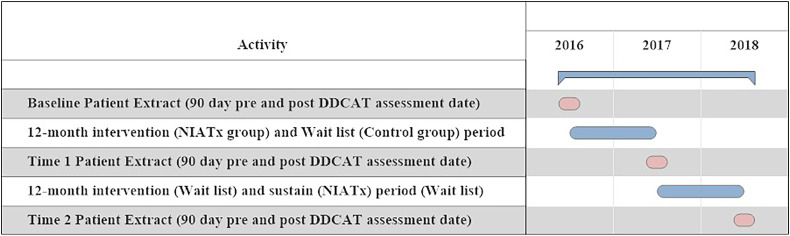
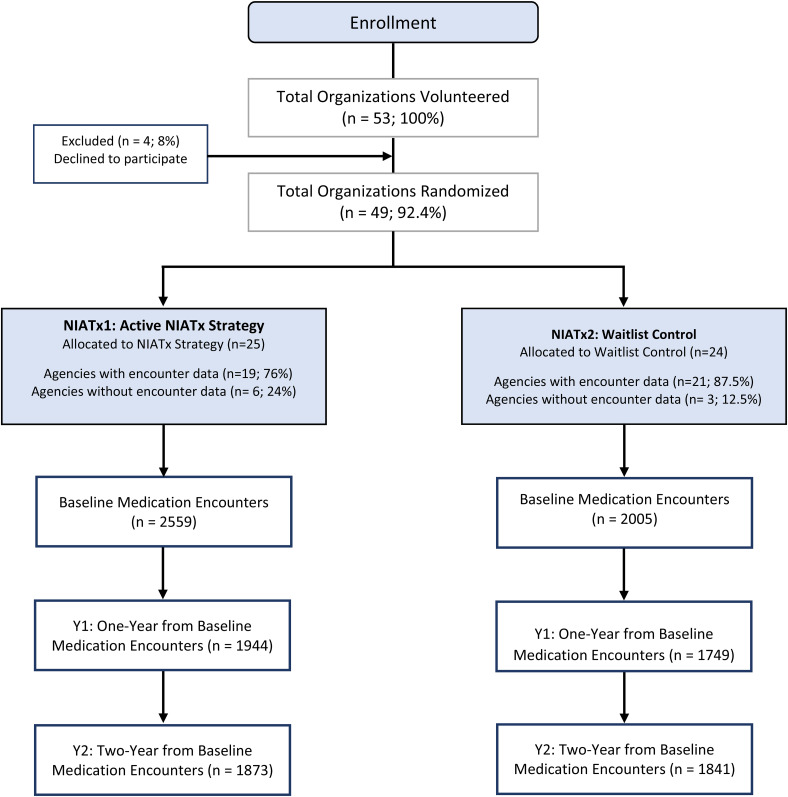
Methods: This study represents a secondary analysis of data from the NIATx project. Forty-nine agencies were randomized to Cohort1 (active implementation group, receiving the NIATx strategy [n=25]) or Cohort2 (waitlist control group [n=24]). Data were collected at three time points (Baseline, Year1 and Year2). A two-level (patient within agency) multinomial logistic regression model investigated the effects of implementation strategy condition on one of four medication outcomes: both medication types, only psychotropic medication, only addiction medication, or neither medication type. A per-protocol analysis included time, NIATx fidelity, and agency focus as predictors.
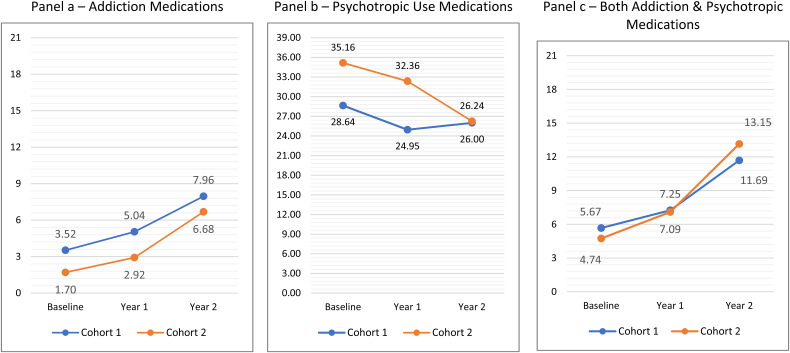
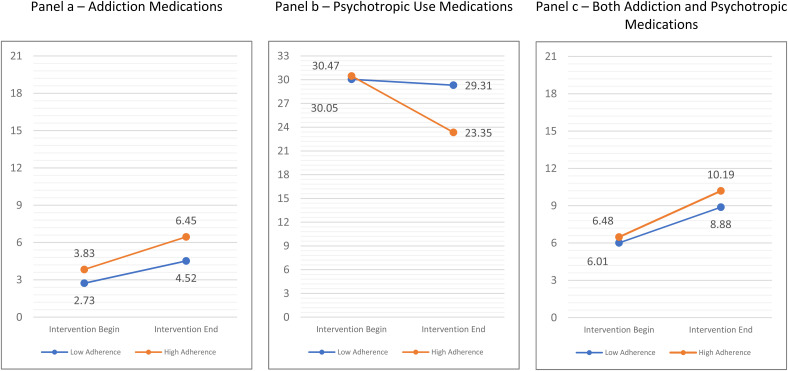
Results: The intent-to-treat analysis found a statistically significant change in access to addiction versus neither medication, but Cohort1 compared to Cohort2 at Year1 showed no differences. Changes were associated with the experimental intervention and occurred in the transition from Year 1 to Year 2, where greater increases were seen for agencies in Cohort2 versus Cohort1. The per-protocol analysis showed increased access to both medications and addiction medications from pre- to post-intervention for agencies in both cohorts; however, differences in change between high- and low-implementation agencies were not significant.
Conclusions: Access to integrated services for people with CODs is a long-standing problem. NIATx implementation strategies had limited effectiveness in improving medication access for individuals with CODs. Implementation strategy adherence is associated with increased medication access.
Keywords: NIATx; access to medications; addiction medications; co-occurring disorders; implementation fidelity; implementation strategy; integrated care; psychotropic medications; quality improvement; substance abuse treatment.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Wait No Longer: Reducing Medication Wait-Times for Individuals with Co-Occurring Disorders.J Dual Diagn. 2022 Apr-Jun;18(2):101-110. doi: 10.1080/15504263.2022.2052225. Epub 2022 Apr 7. J Dual Diagn. 2022. PMID: 35387577 Free PMC article. Clinical Trial.
-
Using NIATx strategies to implement integrated services in routine care: a study protocol.BMC Health Serv Res. 2018 Jun 8;18(1):431. doi: 10.1186/s12913-018-3241-4. BMC Health Serv Res. 2018. PMID: 29884164 Free PMC article.
-
Implementing integrated services in routine behavioral health care: primary outcomes from a cluster randomized controlled trial.BMC Health Serv Res. 2019 Oct 24;19(1):749. doi: 10.1186/s12913-019-4624-x. BMC Health Serv Res. 2019. PMID: 31651302 Free PMC article. Clinical Trial.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
-
Prevention of suicide and attempted suicide in Denmark. Epidemiological studies of suicide and intervention studies in selected risk groups.Dan Med Bull. 2007 Nov;54(4):306-69. Dan Med Bull. 2007. PMID: 18208680 Review.
Cited by
-
Strategies to recruit rural primary care providers to implement a medication for opioid use disorder (MOUD) focused integrated care model.Implement Res Pract. 2023 Feb 19;4:26334895231152808. doi: 10.1177/26334895231152808. eCollection 2023 Jan-Dec. Implement Res Pract. 2023. PMID: 37091535 Free PMC article.
-
Stepped implementation-to-target: a study protocol of an adaptive trial to expand access to addiction medications.Implement Sci. 2022 Sep 29;17(1):64. doi: 10.1186/s13012-022-01239-y. Implement Sci. 2022. PMID: 36175963 Free PMC article.
-
Adapting the stages of implementation completion to an evidence-based implementation strategy: The development of the NIATx stages of implementation completion.Implement Res Pract. 2023 Sep 19;4:26334895231200379. doi: 10.1177/26334895231200379. eCollection 2023 Jan-Dec. Implement Res Pract. 2023. PMID: 37790170 Free PMC article.
References
-
- Assefa M. T., Ford J. H., Osborne E., McIlvaine A., King A., Campbell K., Jo B., McGovern M. P. (2019). Implementing integrated services in routine behavioral health care: primary outcomes from a cluster randomized controlled trial. BMC Health Serv Res,19(1), 749. 10.1186/s12913-019-4624-x - DOI - PMC - PubMed
-
- Baker A. L., Kavanagh D. J., Kay-Lambkin F. J., Hunt S. A., Lewin T. J., Carr V. J., Connolly J. (2010). Randomized controlled trial of cognitive-behavioural therapy for coexisting depression and alcohol problems: Short-term outcome. Addiction, 105(1), 87–99. 10.1111/j.1360-0443.2009.02757.x - DOI - PubMed
-
- Belenko S., Visher C., Pearson F., Swan H., Pich M., O’Connell D., Dembo R., Frisman L., Hamilton L., Willett J. (2017). Efficacy of structured organizational change intervention on HIV testing in correctional facilities. AIDS Education and Prevention, 29(3), 241–255. 10.1521/aeap.2017.29.3.241 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical