

Noninvasive Prediction of Outcomes in Autoimmune Hepatitis-Related Cirrhosis
- PMID: 34989164
- PMCID: PMC9134802
- DOI: 10.1002/hep4.1889
Noninvasive Prediction of Outcomes in Autoimmune Hepatitis-Related Cirrhosis
Abstract
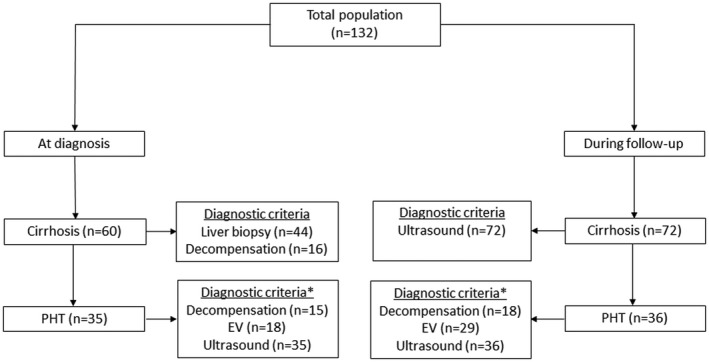
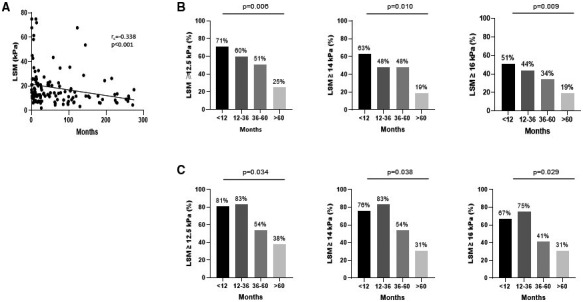
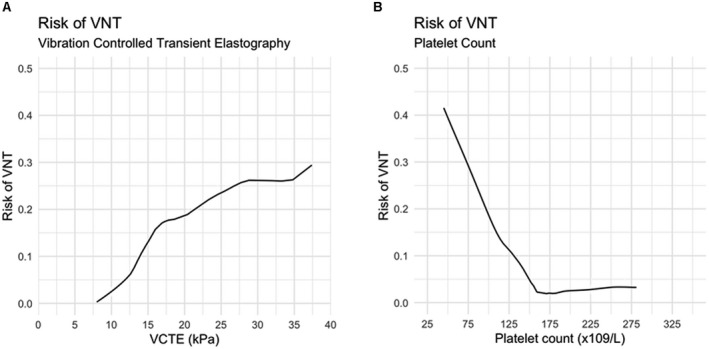
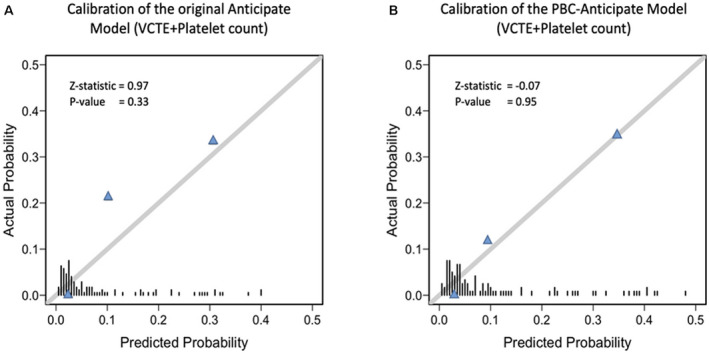
The value of noninvasive tools in the diagnosis of autoimmune hepatitis (AIH)-related cirrhosis and the prediction of clinical outcomes is largely unknown. We sought to evaluate (1) the utility of liver stiffness measurement (LSM) in the diagnosis of cirrhosis and (2) the performance of the Sixth Baveno Consensus on Portal Hypertension (Baveno VI), expanded Baveno VI, and the ANTICIPATE models in predicting the absence of varices needing treatment (VNT). A multicenter cohort of 132 patients with AIH-related cirrhosis was retrospectively analyzed. LSM and endoscopies performed at the time of cirrhosis diagnosis were recorded. Most of the patients were female (66%), with a median age of 54 years. Only 33%-49% of patients had a LSM above the cutoff points described for the diagnosis of AIH-related cirrhosis (12.5, 14, and 16 kPa). Patients with portal hypertension (PHT) had significantly higher LSM than those without PHT (15.7 vs. 11.7 kPa; P = 0.001), but 39%-52% of patients with PHT still had LSM below these limits. The time since AIH diagnosis negatively correlated with LSM, with longer time being significantly associated with a lower proportion of patients with LSM above these cutoffs. VNT was present in 12 endoscopies. The use of the Baveno VI, expanded Baveno VI criteria, and the ANTICIPATE model would have saved 46%-63% of endoscopies, but the latter underpredicted the risk of VNT. Conclusions: LSM cutoff points do not have a good discriminative capacity for the diagnosis of AIH-related cirrhosis, especially long-term after treatment initiation. Noninvasive tools are helpful to triage patients for endoscopy.
© 2022 The Authors. Hepatology Communications published by Wiley Periodicals LLC on behalf of the American Association for the Study of Liver Diseases.
Figures
References
-
- European Association for the Study of the Liver . EASL Clinical Practice Guidelines: autoimmune hepatitis. J Hepatol 2015;63:971‐1004. - PubMed
-
- Werner M, Prytz H, Ohlsson B, Almer S, Bjornsson E, Bergquist A, et al. Epidemiology and the initial presentation of autoimmune hepatitis in Sweden: a nationwide study. Scand J Gastroenterol 2008;43:1232‐1240. - PubMed
-
- Dhaliwal HK, Hoeroldt BS, Dube AK, McFarlane E, Underwood JCE, Karajeh MA, et al. Long‐term prognostic significance of persisting histological activity despite biochemical remission in autoimmune hepatitis. Am J Gastroenterol 2015;110:993‐999. - PubMed
-
- Hartl J, Ehlken H, Sebode M, Peiseler M, Krech T, Zenouzi R, et al. Usefulness of biochemical remission and transient elastography in monitoring disease course in autoimmune hepatitis. J Hepatol 2018;68:754‐763. - PubMed
-
- Hartl J, Denzer U, Ehlken H, Zenouzi R, Peiseler M, Sebode M, et al. Transient elastography in autoimmune hepatitis: timing determines the impact of inflammation and fibrosis. J Hepatol 2016;65:769‐775. - PubMed
