

Executive Summary of Recommendations and Expert Consensus for Plasma and Platelet Transfusion Practice in Critically Ill Children: From the Transfusion and Anemia EXpertise Initiative-Control/Avoidance of Bleeding (TAXI-CAB)
- PMID: 34989711
- PMCID: PMC8820267
- DOI: 10.1097/PCC.0000000000002851
Executive Summary of Recommendations and Expert Consensus for Plasma and Platelet Transfusion Practice in Critically Ill Children: From the Transfusion and Anemia EXpertise Initiative-Control/Avoidance of Bleeding (TAXI-CAB)
Abstract
Objectives: Critically ill children frequently receive plasma and platelet transfusions. We sought to determine evidence-based recommendations, and when evidence was insufficient, we developed expert-based consensus statements about decision-making for plasma and platelet transfusions in critically ill pediatric patients.
Design: Systematic review and consensus conference series involving multidisciplinary international experts in hemostasis, and plasma/platelet transfusion in critically ill infants and children (Transfusion and Anemia EXpertise Initiative-Control/Avoidance of Bleeding [TAXI-CAB]).
Setting: Not applicable.
Patients: Children admitted to a PICU at risk of bleeding and receipt of plasma and/or platelet transfusions.
Interventions: None.
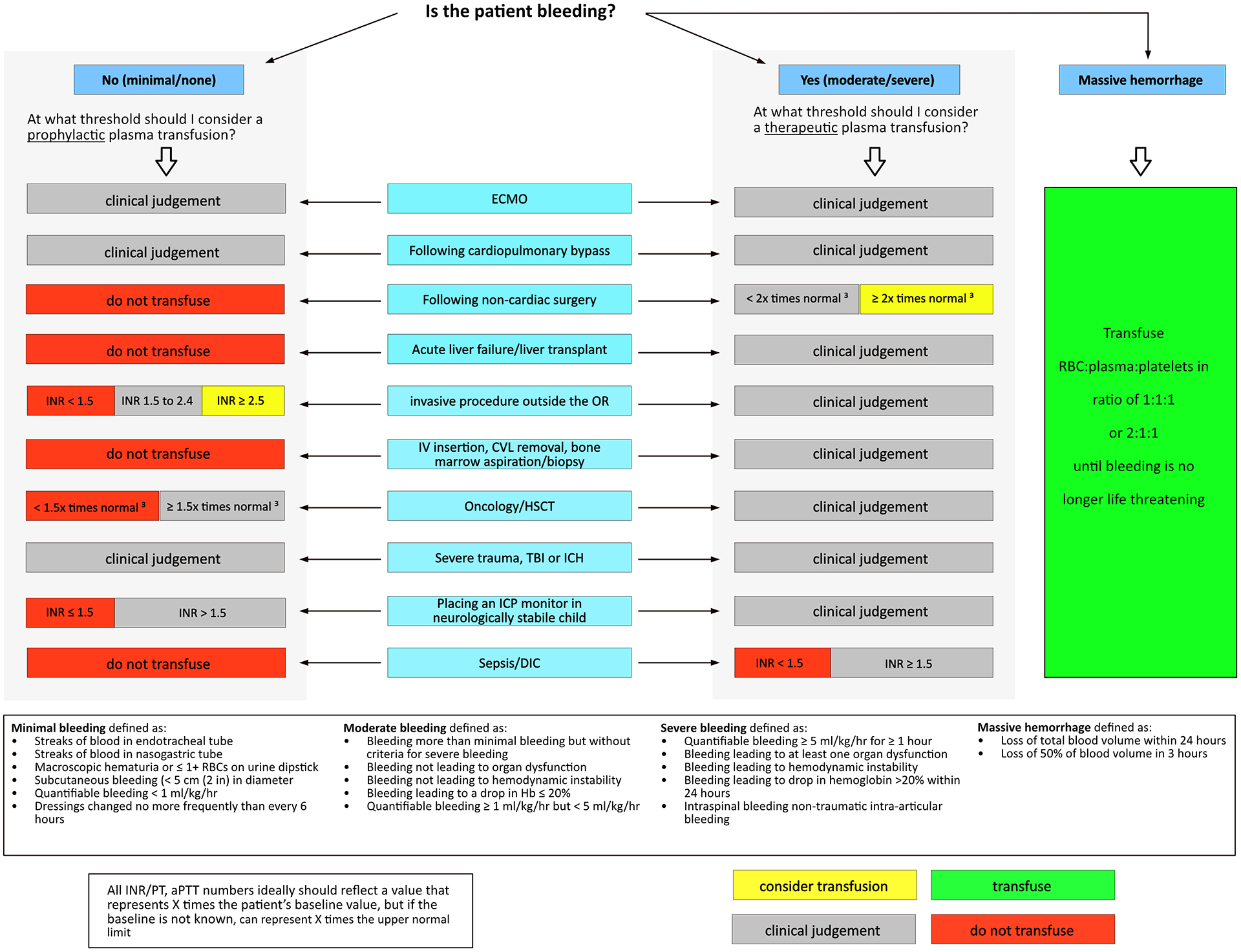
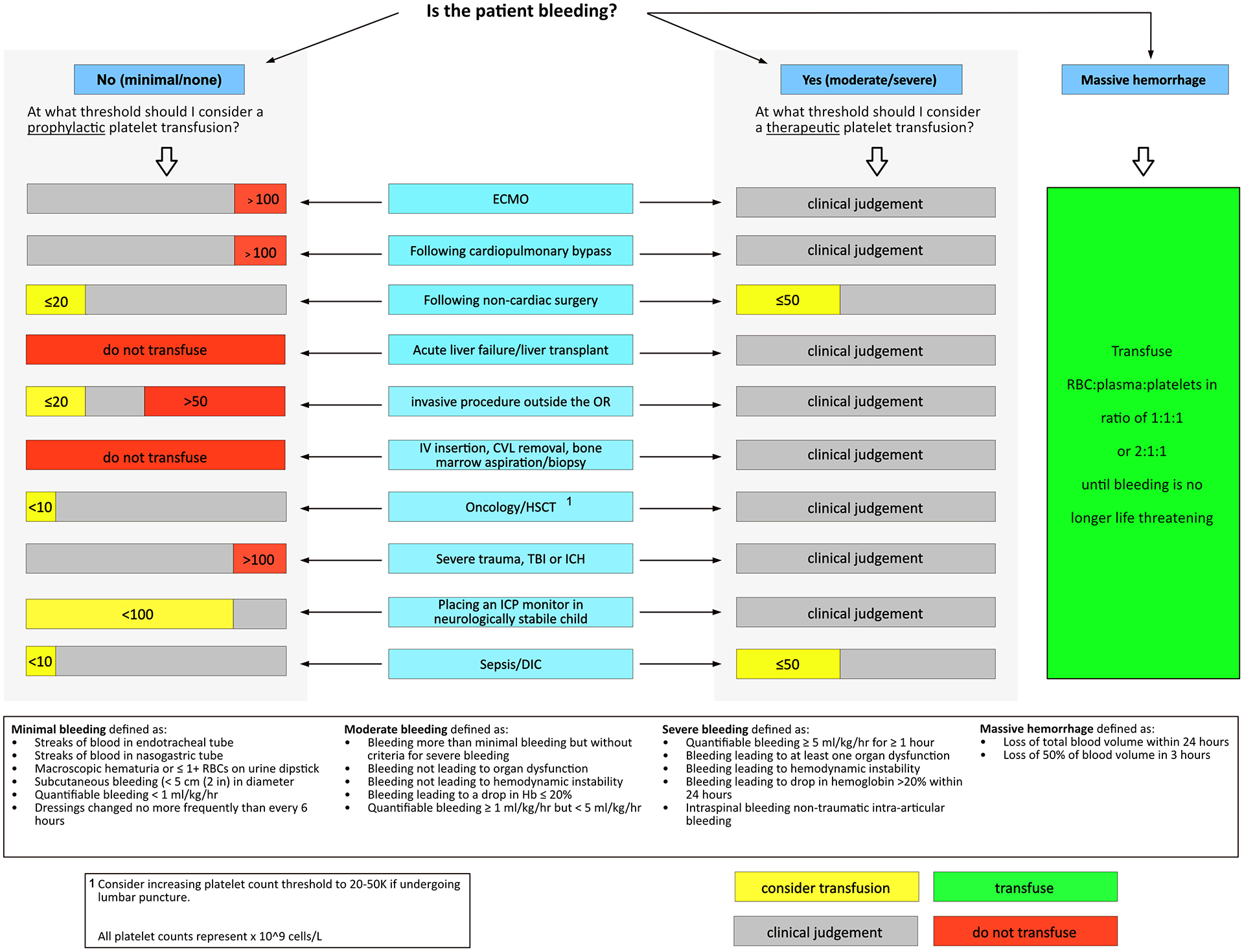
Measurements and main results: A panel of 29 experts in methodology, transfusion, and implementation science from five countries and nine pediatric subspecialties completed a systematic review and participated in a virtual consensus conference series to develop recommendations. The search included MEDLINE, EMBASE, and Cochrane Library databases, from inception to December 2020, using a combination of subject heading terms and text words for concepts of plasma and platelet transfusion in critically ill children. Four graded recommendations and 49 consensus expert statements were developed using modified Research and Development/UCLA and Grading of Recommendations, Assessment, Development, and Evaluation methodology. We focused on eight subpopulations of critical illness (1, severe trauma, intracranial hemorrhage, or traumatic brain injury; 2, cardiopulmonary bypass surgery; 3, extracorporeal membrane oxygenation; 4, oncologic diagnosis or hematopoietic stem cell transplantation; 5, acute liver failure or liver transplantation; 6, noncardiac surgery; 7, invasive procedures outside the operating room; 8, sepsis and/or disseminated intravascular coagulation) as well as laboratory assays and selection/processing of plasma and platelet components. In total, we came to consensus on four recommendations, five good practice statements, and 44 consensus-based statements. These results were further developed into consensus-based clinical decision trees for plasma and platelet transfusion in critically ill pediatric patients.
Conclusions: The TAXI-CAB program provides expert-based consensus for pediatric intensivists for the administration of plasma and/or platelet transfusions in critically ill pediatric patients. There is a pressing need for primary research to provide more evidence to guide practitioners.
Copyright © 2021 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Conflict of interest statement
Drs. Nellis, Bateman, Bembea, and Russell received support for article research from the National Institutes of Health. Dr. Bembea’s institution received funding from the National Institute of Neurologic Disorders and Stroke (R01NS106292), the National Institute of Child Health and Human Development, and Grifols Investigator Sponsored Research Grant. Dr. Nishijima received funding from Bristol Myers Squibb. Dr. Emani received funding from Cheisi Pharmaceuticals. Dr. Haas received funding from Octapharma. Dr. Goel received funding from the National Heart, Lung, and Blood Institute and Rigel Pharmaceuticals. Dr. Crighton disclosed that she is employed by Royal Children’s Hospital of Melbourne, Australia and that she was the Australian and New Zealand Society of Blood Transfusion President. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- White LJ, Fredericks R, Mannarino CN, Janofsky S, Faustino EVS. Epidemiology of bleeding in critically ill children. J Pediatr 2017, 184:114–119. - PubMed
-
- Karam O, Lacroix J, Robitaille N, Rimensberger PC, Tucci M. Association between plasma transfusions and clinical outcome in critically ill children: a prospective observational study. Vox Sang 2013, 104:342–349. - PubMed
-
- Kleinman S, Chan P, Robillard P. Risks associated with transfusion of cellular blood components in Canada. Transf Med Rev 2003, 17:120–162. - PubMed
