

Comparison of Prophylactic Intravenous Antibiotic Regimens After Endoprosthetic Reconstruction for Lower Extremity Bone Tumors: A Randomized Clinical Trial
- PMID: 34989778
- PMCID: PMC8739829
- DOI: 10.1001/jamaoncol.2021.6628
Comparison of Prophylactic Intravenous Antibiotic Regimens After Endoprosthetic Reconstruction for Lower Extremity Bone Tumors: A Randomized Clinical Trial
Abstract
Importance: The use of perioperative, prophylactic, intravenous antibiotics is standard practice to reduce the risk of surgical site infection after oncologic resection and complex endoprosthetic reconstruction for lower extremity bone tumors. However, evidence guiding the duration of prophylactic treatment remains limited.
Objective: To assess the effect of a 5-day regimen of postoperative, prophylactic, intravenous antibiotics compared with a 1-day regimen on the rate of surgical site infections within 1 year after surgery.
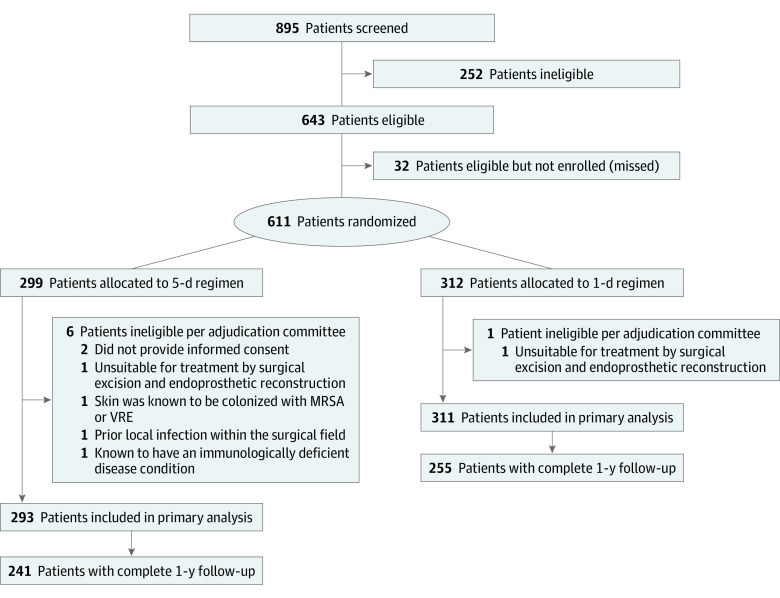
Design, setting, and participants: This randomized clinical superiority trial was performed at 48 clinical sites in 12 countries from January 1, 2013, to October 29, 2019. The trial included patients with a primary bone tumor or a soft tissue sarcoma that had invaded the femur or tibia or oligometastatic bone disease of the femur or tibia with expected survival of at least 1 year who required surgical management by excision and endoprosthetic reconstruction. A total of 611 patients were enrolled, and 7 were excluded for ineligibility.
Interventions: A 1- or 5-day regimen of postoperative prophylactic intravenous cephalosporin (cefazolin or cefuroxime) that began within 8 hours after skin closure and was administered every 8 hours thereafter. Those randomized to the 1-day regimen received identical saline doses every 8 hours for the remaining 4 days; patients, care providers, and outcomes assessors were blinded to treatment regimen.
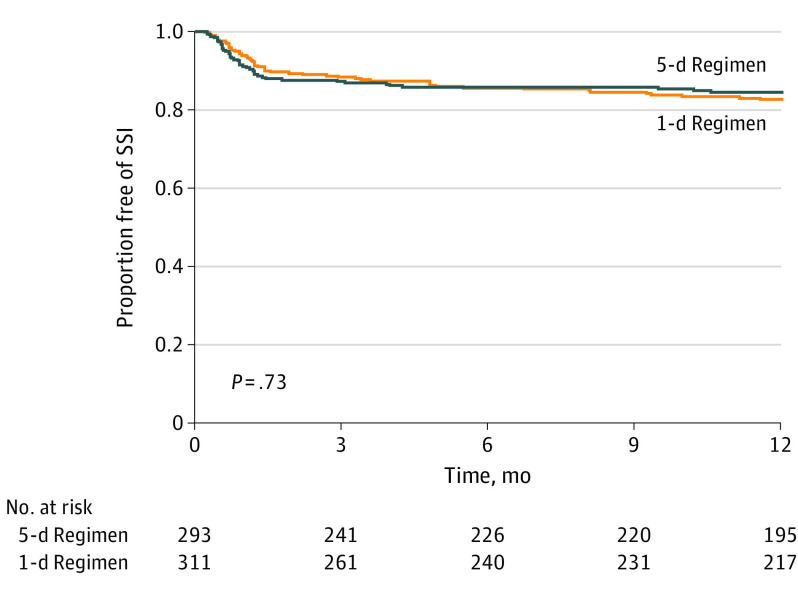
Main outcomes and measures: The primary outcome in this superiority trial was a surgical site infection (superficial incisional, deep incisional, or organ space) classified according to the criteria established by the Centers for Disease Control and Prevention within 1 year after surgery. Secondary outcomes included antibiotic-related complications, unplanned additional operations, oncologic and functional outcomes, and mortality.
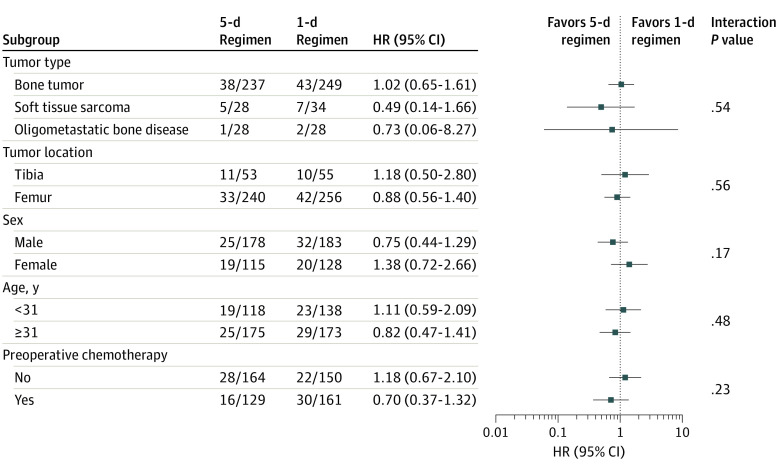
Results: Of the 604 patients included in the final analysis (mean [SD] age, 41.2 [21.9] years; 361 [59.8%] male; 114 [18.9%] Asian, 43 [7.1%] Black, 34 [5.6%] Hispanic, 15 [2.5%] Indigenous, 384 [63.8%] White, and 12 [2.0%] other), 293 were randomized to a 5-day regimen and 311 to a 1-day regimen. A surgical site infection occurred in 44 patients (15.0%) allocated to the 5-day regimen and in 52 patients (16.7%) allocated to the 1-day regimen (hazard ratio, 0.93; 95% CI, 0.62-1.40; P = .73). Antibiotic-related complications occurred in 15 patients (5.1%) in the 5-day regimen and in 5 patients (1.6%) allocated to the 1-day regimen (hazard ratio, 3.24; 95% CI, 1.17-8.98; P = .02). Other secondary outcomes did not differ significantly between treatment groups.
Conclusions and relevance: This randomized clinical trial did not confirm the superiority of a 5-day regimen of postoperative intravenous antibiotics over a 1-day regimen in preventing surgical site infections after surgery for lower extremity bone tumors that required an endoprosthesis. The 5-day regimen group had significantly more antibiotic-related complications.
Trial registration: ClinicalTrials.gov Identifier: NCT01479283.
Conflict of interest statement
Figures
Comment in
-
Antibiotic Prophylaxis of Surgical Site Infections-A Double-edged Sword for Oncology Patients?JAMA Oncol. 2022 Mar 1;8(3):340-342. doi: 10.1001/jamaoncol.2021.6619. JAMA Oncol. 2022. PMID: 34989806 No abstract available.
-
Prophylactic Antibiotic Regimens in Tumor Resection Surgery Involving a Prosthesis.JAMA Oncol. 2022 Aug 1;8(8):1222. doi: 10.1001/jamaoncol.2022.2056. JAMA Oncol. 2022. PMID: 35737358 No abstract available.
-
Prophylactic Antibiotic Regimens in Tumor Resection Surgery Involving a Prosthesis-Reply.JAMA Oncol. 2022 Aug 1;8(8):1222-1223. doi: 10.1001/jamaoncol.2022.2059. JAMA Oncol. 2022. PMID: 35737365 No abstract available.
-
The PARITY Trial: A Sea Change in Musculoskeletal Oncology Research.J Bone Joint Surg Am. 2023 Jul 19;105(14):1053. doi: 10.2106/JBJS.23.00433. Epub 2023 May 9. J Bone Joint Surg Am. 2023. PMID: 37466484 No abstract available.
