

Effectiveness of a Novel ω-3 Krill Oil Agent in Patients With Severe Hypertriglyceridemia: A Randomized Clinical Trial
- PMID: 34989797
- PMCID: PMC8739762
- DOI: 10.1001/jamanetworkopen.2021.41898
Effectiveness of a Novel ω-3 Krill Oil Agent in Patients With Severe Hypertriglyceridemia: A Randomized Clinical Trial
Abstract
Importance: Intense interest exists in novel ω-3 formulations with high bioavailability to reduce blood triglyceride (TG) levels.
Objective: To determine the phase 3 efficacy and safety of a naturally derived krill oil with eicosapentaenoic acid and docosahexaenoic acid as both phospholipid esters (PLs) and free fatty acids (FFAs) (ω-3-PL/FFA [CaPre]), measured by fasting TG levels and other lipid parameters in severe hypertriglyceridemia.
Design, setting, and participants: This study pooled the results of 2 identical randomized, double-blind, placebo-controlled trials. TRILOGY 1 (Study of CaPre in Lowering Very High Triglycerides) enrolled participants at 71 US centers from January 23, 2018, to November 20, 2019; TRILOGY 2 enrolled participants at 93 US, Canadian, and Mexican centers from April 6, 2018, to January 9, 2020. Patients with fasting TG levels from 500 to 1500 mg/dL, with or without stable treatment with statins, fibrates, or other agents to lower cholesterol levels, were eligible to participate.
Interventions: Randomization (2.5:1.0) to ω-3-PL/FFA, 4 g/d, vs placebo (cornstarch) for 26 weeks.
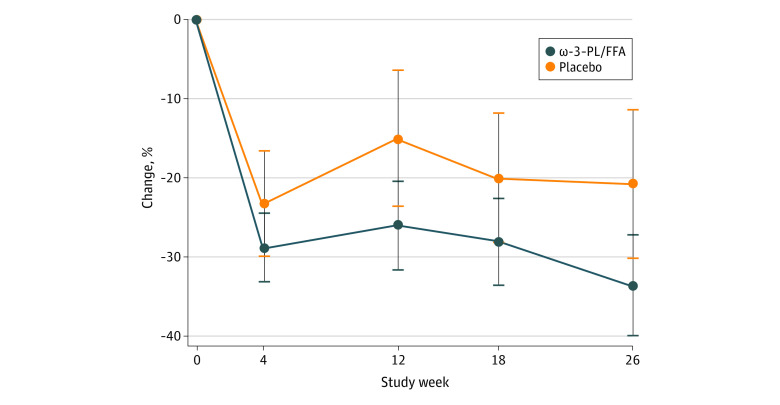
Main outcomes and measures: The primary outcome was the mean percentage of change in TG levels at 12 weeks; persistence at 26 weeks was the key secondary outcome. Other prespecified secondary outcomes were effects on levels of non-high-density lipoprotein cholesterol (non-HDL-C), very-low-density lipoprotein cholesterol (VLDL-C), HDL-C, and low-density lipoprotein cholesterol (LDL-C); safety and tolerability; and TG level changes in prespecified subgroups.
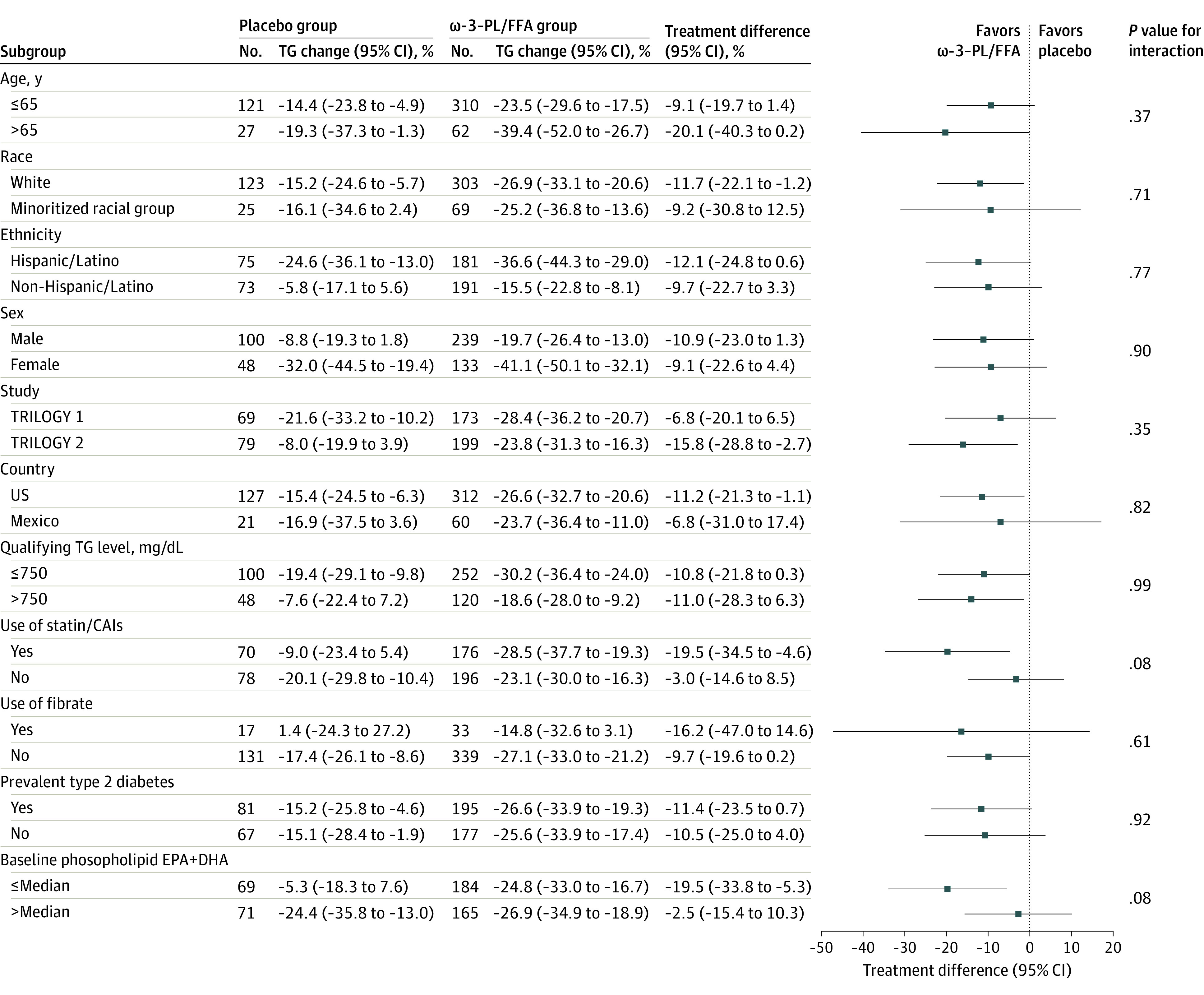
Results: A total of 520 patients were randomized, with a mean (SD) age of 54.9 (11.2) years (339 men [65.2%]), mean (SD) body mass index of 31.5 (5.1), and baseline mean (SD) TG level of 701 (222) mg/dL. Two hundred fifty-six patients (49.2%) were of Hispanic or Latino ethnicity; 275 (52.9%) had diabetes; and 248 (47.7%) were receiving statins. In the intention-to-treat analysis, TG levels were reduced by 26.0% (95% CI, 20.5%-31.5%) in the ω-3-PL/FFA group and 15.1% (95% CI, 6.6%-23.5%) in the placebo group at 12 weeks (mean treatment difference, -10.9% [95% CI, -20.4% to -1.5%]; P = .02), with reductions persisting at 26 weeks (mean treatment difference, -12.7% [95% CI, -23.1% to -2.4%]; P = .02). Compared with placebo, ω-3-PL/FFA had no significant effect at 12 weeks on mean treatment differences for non-HDL-C (-3.2% [95% CI, -8.0% to 1.6%]; P = .18), VLDL-C (-3.8% [95% CI, -12.2% to 4.7%]; P = .38), HDL-C (0.7% [95% CI, -3.7% to 5.1%]; P = .77), or LDL-C (4.5% [95% CI, -5.9% to 14.8%]; P = .40) levels; corresponding differences at 26 weeks were -5.8% (95% CI, -11.3% to -0.3%; P = .04) for non-HDL-C levels, -9.1% (95% CI, -21.5% to 3.2%; P = .15) for VLDL-C levels, 1.9% (95% CI, -4.8% to 8.6%; P = .57) for HDL-C levels, and 6.3% (95% CI, -12.4% to 25.0%; P = .51) for LDL-C levels. Effects on the primary end point did not vary significantly by age, sex, race and ethnicity, country, qualifying TG level, diabetes, or fibrate use but tended to be larger among patients taking statins or cholesterol absorption inhibitors at baseline (mean treatment difference, -19.5% [95% CI, -34.5% to -4.6%]; P = .08 for interaction) and with lower (less than median) baseline blood eicosapentaenoic acid plus docosahexaenoic acid levels (-19.5% [95% CI, -33.8% to -5.3%]; P = .08 for interaction). ω-3-PL/FFA was well tolerated, with a safety profile similar to that of placebo.
Conclusions and relevance: This study found that ω-3 -PL/FFA, a novel krill oil-derived ω-3 formulation, reduced TG levels and was safe and well tolerated in patients with severe hypertriglyceridemia.
Trial registration: ClinicalTrials.gov Identifiers: NCT03398005 and NCT03361501.
Conflict of interest statement
Figures
References
-
- NCD Risk Factor Collaboration (NCD-RisC) . Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. 2017;390(10 113):2627-2642. - PMC - PubMed
-
- Miller M, Stone NJ, Ballantyne C, et al. ; American Heart Association Clinical Lipidology, Thrombosis, and Prevention Committee of the Council on Nutrition, Physical Activity, and Metabolism; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Nursing; Council on the Kidney in Cardiovascular Disease . Triglycerides and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2011;123(20):2292-2333. doi: 10.1161/CIR.0b013e3182160726 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
