

Attributable Mortality of Candida Bloodstream Infections in the Modern Era: A Propensity Score Analysis
- PMID: 34989802
- PMCID: PMC10233239
- DOI: 10.1093/cid/ciac004
Attributable Mortality of Candida Bloodstream Infections in the Modern Era: A Propensity Score Analysis
Abstract
Background: This study quantifies the mortality attributable to Candida bloodstream infections (BSI) in the modern era of echinocandins.
Methods: We conducted a retrospective cohort study of adult patients admitted to Barnes Jewish Hospital, a 1368-bed tertiary care academic hospital, in Saint Louis, Missouri, from 1 February 2012 to 30 April 2019. We identified 626 adult patients with Candida BSI that were frequency-matched with 6269 control patients that had similar Candida BSI risk-factors. The 90-day all-cause mortality attributable to Candida BSI was calculated using three methods-propensity score matching, matching by inverse weighting of propensity score, and stratified analysis by quintile.
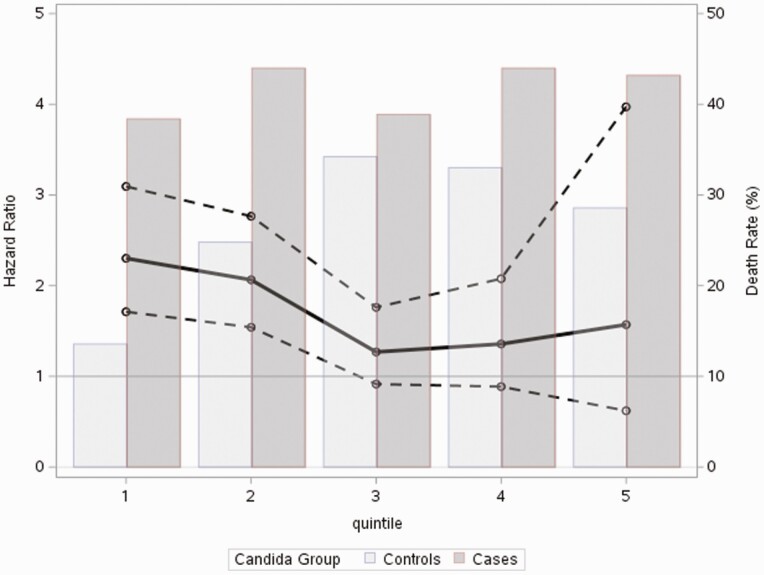
Results: The 90-day crude mortality was 42.4% (269 patients) for Candida BSI cases and 17.1% (1083 patients) for frequency-matched controls. Following propensity score-matching, the attributable risk difference for 90-day mortality was 28.4% with hazard ratio (HR) of 2.12 (95% confidence interval [CI], 1.98-2.25, P < .001). In the stratified analysis, the risk for mortality at 90 days was highest in patients in the lowest risk quintile to develop Candida BSI (hazard ratio [HR] 3.13 (95% CI, 2.33-4.19). Patients in this lowest risk quintile accounted for 81(61%) of the 130 untreated patients with Candida BSI. Sixty-nine percent of untreated patients (57/83) died versus 35% of (49/127) of treated patients (P < .001).
Conclusions: Patients with Candida BSI continue to experience high mortality. Mortality attributable to Candida BSI was more pronounced in patients at lowest risk to develop Candida BSI. A higher proportion of these low-risk patients went untreated, experienced higher mortality, and should be the target of aggressive interventions to ensure timely, effective treatment.
Keywords: Candida; amphotericin; echinocandin; fluconazole; mortality.
© The Author(s) 2022. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. M. O. reports grants and personal fees from Pfizer, grants from Merck and Sanofi. D. S. reports personal stock ownership in AbbVie, Inc. and Bristol-Myers Squibb. W. P. reports grants and personal fees from Merck and Co, personal fees from Gilead Sciences. A. S. reports grants from Astellas Global Development Pharma, Inc., grants and personal fees from Scynexis, grants from Cidara, grants from Mayne Pharma. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Kullberg BJ, Arendrup MC. Invasive candidiasis. N Engl J Med 2015; 373:1445–56. - PubMed
-
- Pappas PG, Lionakis MS, Arendrup MC, Ostrosky-Zeichner L, Kullberg BJ. Invasive candidiasis. Nat Rev Dis Primers 2018; 4:18026. - PubMed
-
- Cornely FB, Cornely OA, Salmanton-Garcia J, et al. Attributable mortality of candidemia after introduction of echinocandins. Mycoses 2020; 63:1373–81. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
