

DeepLensNet: Deep Learning Automated Diagnosis and Quantitative Classification of Cataract Type and Severity
- PMID: 34990643
- PMCID: PMC9038670
- DOI: 10.1016/j.ophtha.2021.12.017
DeepLensNet: Deep Learning Automated Diagnosis and Quantitative Classification of Cataract Type and Severity
Abstract
Purpose: To develop deep learning models to perform automated diagnosis and quantitative classification of age-related cataract from anterior segment photographs.
Design: DeepLensNet was trained by applying deep learning models to the Age-Related Eye Disease Study (AREDS) dataset.
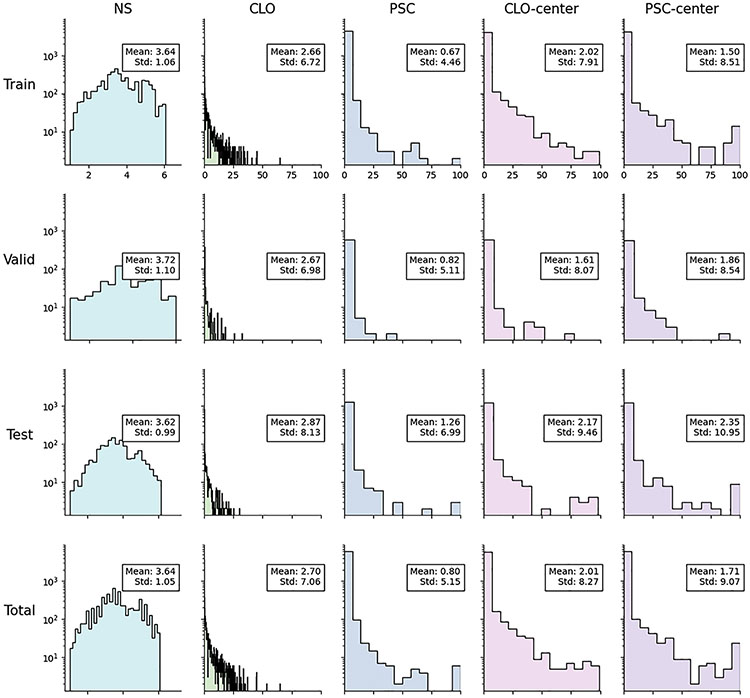
Participants: A total of 18 999 photographs (6333 triplets) from longitudinal follow-up of 1137 eyes (576 AREDS participants).
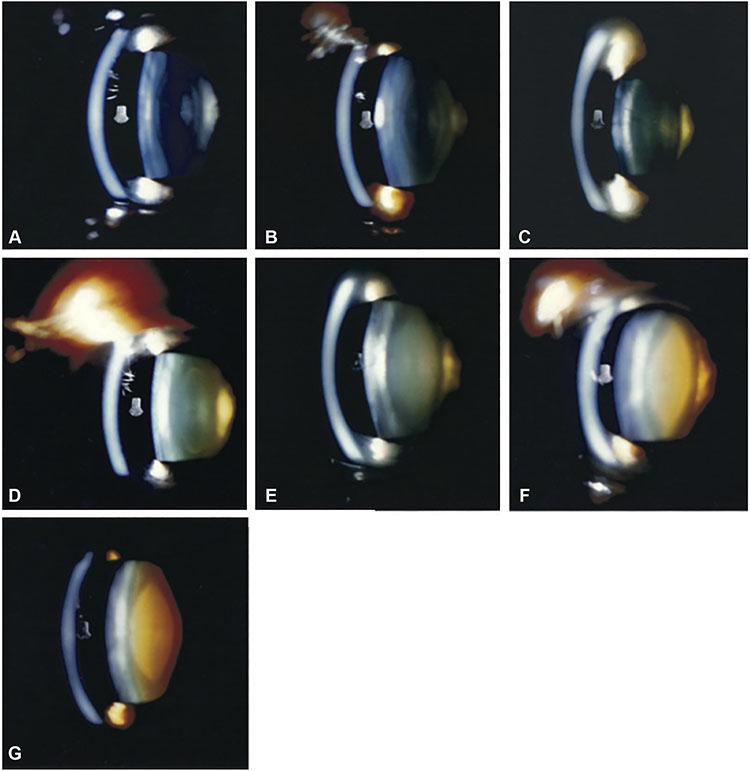
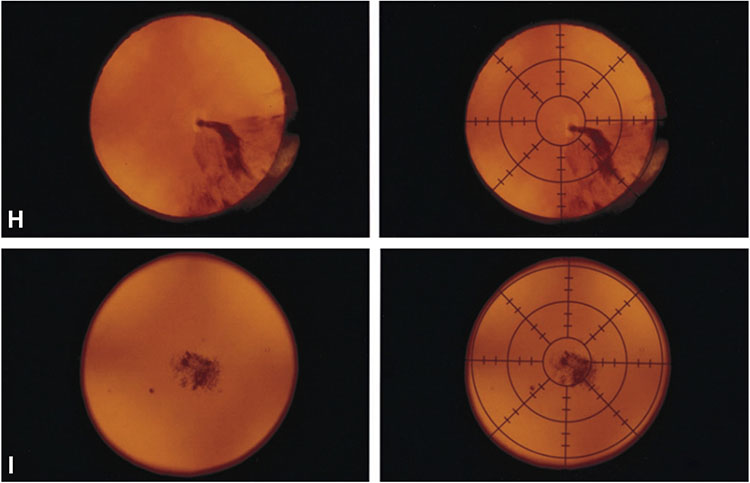
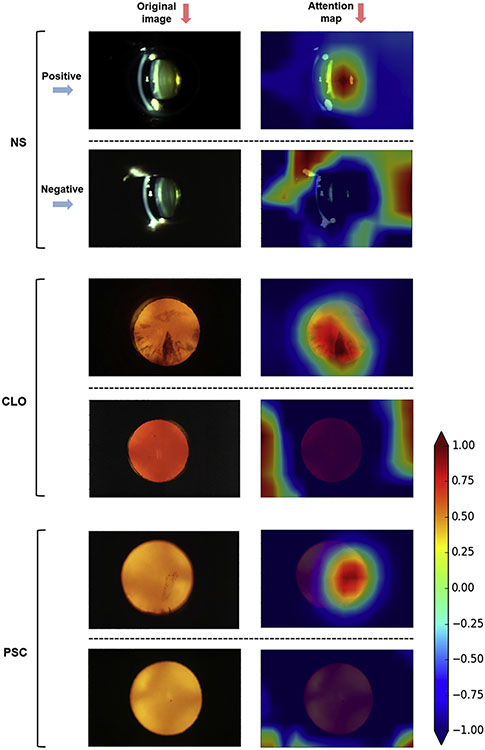
Methods: Deep learning models were trained to detect and quantify nuclear sclerosis (NS; scale 0.9-7.1) from 45-degree slit-lamp photographs and cortical lens opacity (CLO; scale 0%-100%) and posterior subcapsular cataract (PSC; scale 0%-100%) from retroillumination photographs. DeepLensNet performance was compared with that of 14 ophthalmologists and 24 medical students.
Main outcome measures: Mean squared error (MSE).
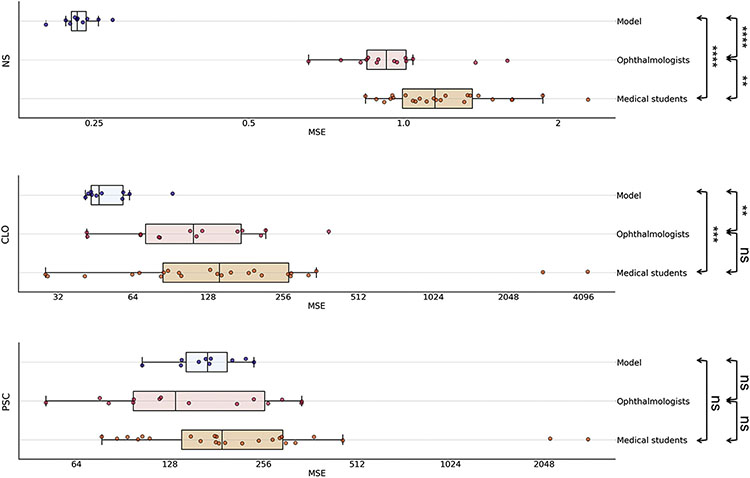
Results: On the full test set, mean MSE for DeepLensNet was 0.23 (standard deviation [SD], 0.01) for NS, 13.1 (SD, 1.6) for CLO, and 16.6 (SD, 2.4) for PSC. On a subset of the test set (substantially enriched for positive cases of CLO and PSC), for NS, mean MSE for DeepLensNet was 0.23 (SD, 0.02), compared with 0.98 (SD, 0.24; P = 0.000001) for the ophthalmologists and 1.24 (SD, 0.34; P = 0.000005) for the medical students. For CLO, mean MSE was 53.5 (SD, 14.8), compared with 134.9 (SD, 89.9; P = 0.003) for the ophthalmologists and 433.6 (SD, 962.1; P = 0.0007) for the medical students. For PSC, mean MSE was 171.9 (SD, 38.9), compared with 176.8 (SD, 98.0; P = 0.67) for the ophthalmologists and 398.2 (SD, 645.4; P = 0.18) for the medical students. In external validation on the Singapore Malay Eye Study (sampled to reflect the cataract severity distribution in AREDS), the MSE for DeepSeeNet was 1.27 for NS and 25.5 for PSC.
Conclusions: DeepLensNet performed automated and quantitative classification of cataract severity for all 3 types of age-related cataract. For the 2 most common types (NS and CLO), the accuracy was significantly superior to that of ophthalmologists; for the least common type (PSC), it was similar. DeepLensNet may have wide potential applications in both clinical and research domains. In the future, such approaches may increase the accessibility of cataract assessment globally. The code and models are available at https://github.com/ncbi/deeplensnet.
Keywords: Artificial intelligence; Automated diagnosis; Cataract; Cortical cataract; Deep learning; Nuclear sclerosis; Posterior subcapsular cataract; Severity classification; Telemedicine; Teleophthalmology.
Copyright © 2022. Published by Elsevier Inc.
Figures
References
-
- Lam D, Rao SK, Ratra V, et al. Cataract. Nat Rev Dis Primers. 2015;1:15014. - PubMed
-
- GBD 2019 Blindness and Vision Impairment Collaborators; Vision Loss Expert Group of the Global Burden of Disease Study. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the Right to Sight: an analysis for the Global Burden of Disease Study. Lancet Glob Health. 2021;9:e144–e160. - PMC - PubMed
-
- Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990-2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5:e1221–e1234. - PubMed
-
- Bastawrous A, Suni AV. Thirty year projected magnitude (to 2050) of near and distance vision impairment and the economic impact if existing solutions are implemented globally. Ophthalmic Epidemiol. 2020;27:115–120. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
