

Using Longitudinally Linked Data to Measure Severe Maternal Morbidity
- PMID: 34991121
- PMCID: PMC8820447
- DOI: 10.1097/AOG.0000000000004641
Using Longitudinally Linked Data to Measure Severe Maternal Morbidity
Abstract
Objective: To assess whether application of a standard algorithm to hospitalizations in the prenatal and postpartum (42 days) periods increases identification of severe maternal morbidity (SMM) beyond analysis of only the delivery event.
Methods: We performed a retrospective cohort study using data from the PELL (Pregnancy to Early Life Longitudinal) database, a Massachusetts population-based data system that links records from birth certificates to delivery hospital discharge records and nonbirth hospital records for all birthing individuals. We included deliveries from January 1, 2009, to December 31, 2018, distinguishing between International Classification of Diseases Ninth (ICD-9) and Tenth Revision (ICD-10) coding. We applied the modified Centers for Disease Control and Prevention algorithm for SMM used by the Alliance for Innovation on Maternal Health to hospitalizations across the antenatal period through 42 days postpartum. Morbidity was examined both with and without blood transfusion.
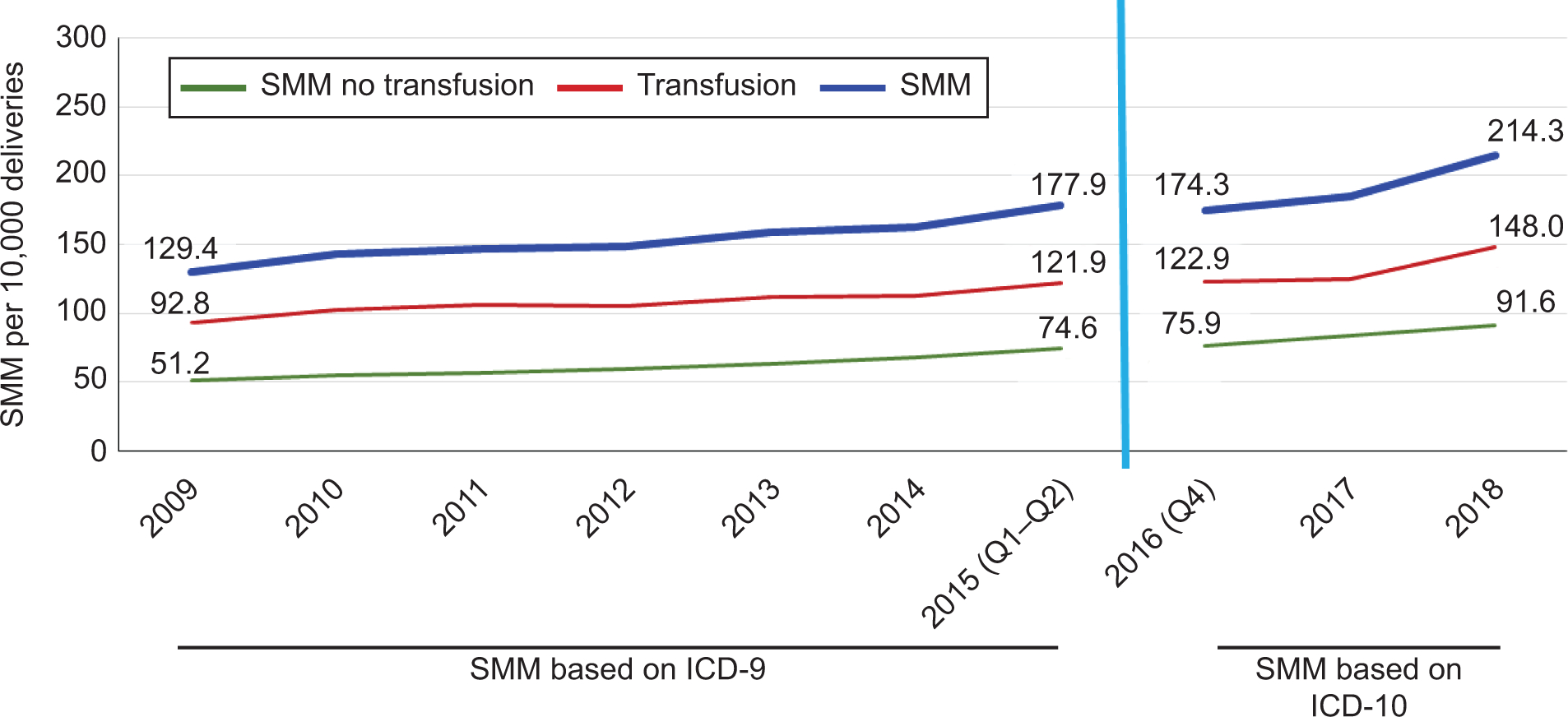
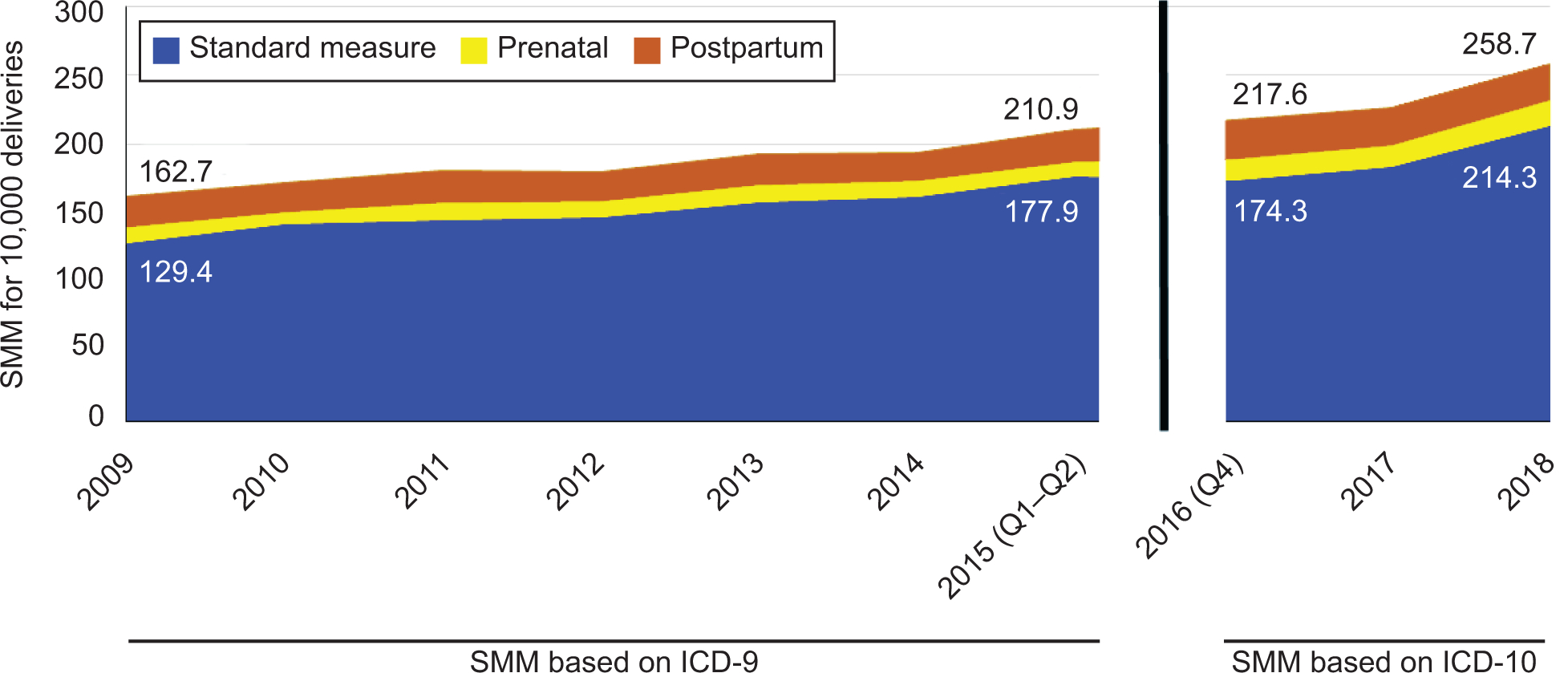
Results: Overall, 594,056 deliveries were included in the analysis, and 3,947 deliveries met criteria for SMM at delivery without transfusion and 9,593 with transfusion for aggregate rates of 150.1 (95% CI 146.7-153.5) using ICD-9 codes and 196.6 (95% CI 189.5-203.7) using ICD-10 codes per 10,000 deliveries. Severe maternal morbidity at birth increased steadily across both ICD-9 and ICD-10 from 129.4 in 2009 (95% CI 126.2-132.6) using ICD-9 to 214.3 per 10,000 (95% CI 206.9-221.8) in 2018 using ICD-10. Adding prenatal and postpartum hospitalizations increased cases by 21.9% under both ICD-9 and ICD-10, resulting in a 2018 rate of 258.7 per 10,000 (95% CI 250.5-266.9). The largest increase in detected morbidity in the prenatal or postpartum time period was attributed to sepsis cases.
Conclusion: Inclusion of prenatal and postpartum hospitalizations in the identification of SMM resulted in increased ascertainment of morbid events. These results suggest a need to ensure surveillance of care quality activities beyond the birth event.
Copyright © 2022 by the American College of Obstetricians and Gynecologists. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Financial Disclosure Elysia Larson disclosed receiving funding from the World Bank and the Harvard T.H. Chan School of Public Health. Audra Meadows disclosed receiving funding from the Institute for Health Care Improvement, Better Maternal Outcomes (consultancy), the Black Birth Equity Community Advisory Board, and the Institute for Perinatal Quality Improvement (consultancy). The other authors did not report any potential conflicts of interest.
Figures
Comment in
-
Identifying Cases of Severe Maternal Morbidity: Moving Beyond the Delivery Hospitalization.Obstet Gynecol. 2022 Feb 1;139(2):163-164. doi: 10.1097/AOG.0000000000004665. Obstet Gynecol. 2022. PMID: 34991143 No abstract available.
References
-
- Weil A, Reichert Ae. Reversing the U.S. Maternal Mortality Crisis: A Report of the Aspen Health Strategy Group. Washington, D.C.2021.
-
- Hoyert D Maternal mortality rates in the United States, 2019. NCHS Health E-Stats. 2021. DOI: 10.15620/cdc:103855. - DOI
-
- Geller SE, Rosenberg D, Cox SM, Kilpatrick S. Defining a conceptual framework for near-miss maternal morbidity. Journal of the American Medical Women’s Association (1972). 2002;57(3):135–139. - PubMed
-
- Callaghan WM, Creanga A, Kuklina E. Severe maternal morbidity among delivery and postpartum hospitalizations in the United States. Obstet Gynecol. 2012;120:1029–1036. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
