

Pregnancy-Associated Deaths Due to Drugs, Suicide, and Homicide in the United States, 2010-2019
- PMID: 34991132
- PMCID: PMC8849543
- DOI: 10.1097/AOG.0000000000004649
Pregnancy-Associated Deaths Due to Drugs, Suicide, and Homicide in the United States, 2010-2019
Abstract
Objective: To estimate the prevalence of pregnancy-associated deaths due to drugs, suicide, and homicide nationwide from 2010 to 2019.
Methods: Using U.S. death certificate records from 2010 to 2019 for 33 states plus the District of Columbia, we identified pregnancy-associated deaths using the pregnancy checkbox and International Classification of Diseases, Tenth Revision codes, calculated pregnancy-associated death ratios, and categorized deaths by cause, timing relative to pregnancy, race or ethnicity, and age.
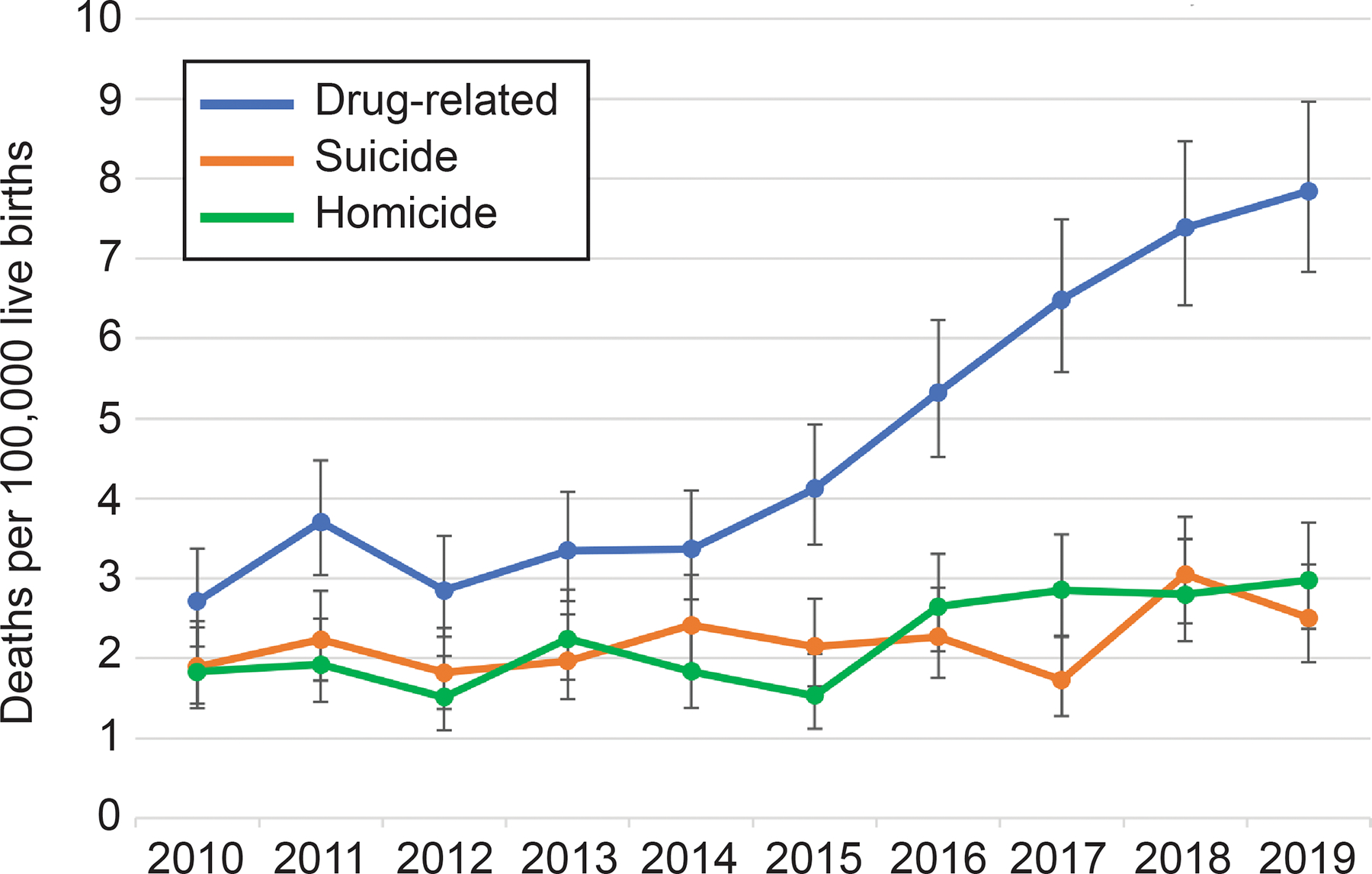
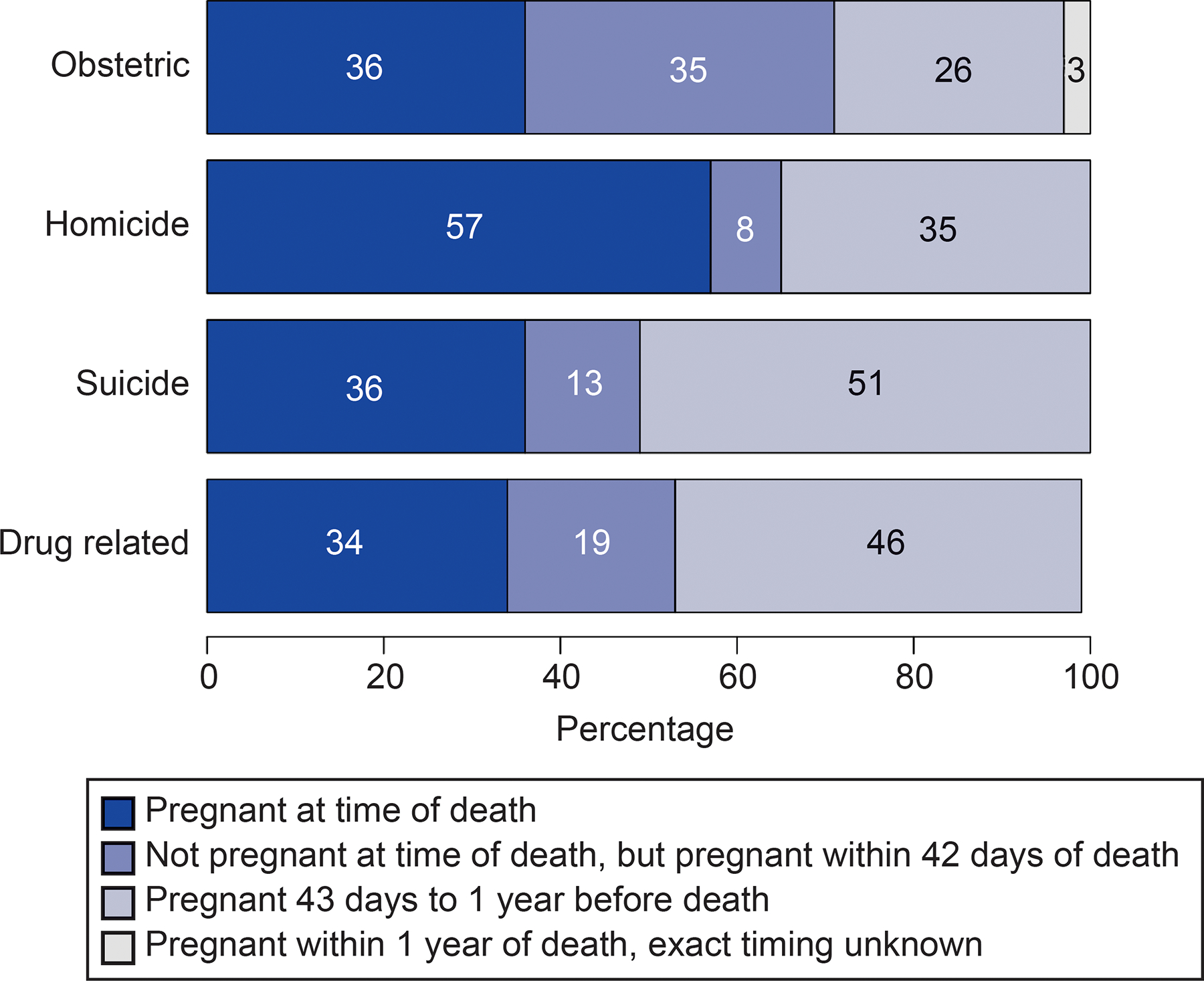
Results: Of 11,782 pregnancy-associated deaths identified between 2010 and 2019, 11.4% were due to drugs, 5.4% were due to suicide, and 5.4% were due to homicide, whereas 59.3% were due to obstetric causes and the remaining 18.5% were due to other causes. Drug-related deaths, suicide, and homicide accounted for 22.2% of pregnancy-associated deaths. All three causes of death increased over the study period, with drug-related pregnancy-associated deaths increasing 190%. Homicide during pregnancy and drug-related deaths, suicides, and homicide in the late postpartum period (43-365 days) accounted for a larger proportion of all deaths in these time periods than the contribution of these causes to all deaths among females of reproductive age. Pregnant and postpartum people identified as non-Hispanic American Indian or Alaska Native were at highest risk of drug-related and suicide death, and people identified as non-Hispanic Black were at highest risk of homicide.
Conclusion: Deaths due to drug use, suicide, and homicide constitute more than one fifth of all deaths during pregnancy and the first year postpartum. Drug-related deaths and homicides have increased over the past decade. Substantial racial and ethnic inequities in these deaths exist.
Copyright © 2022 by the American College of Obstetricians and Gynecologists. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Financial Disclosure Alison Gemmill reports money was paid to her from the World Health Organization and Avenir Health. The other authors did not report any potential conflicts of interest.
Figures
References
-
- World Health Organization. Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Geneva: World Health Organization; 2019. Accessed July 6, 2021. https://www.who.int/reproductivehealth/publications/maternal-mortality-2...
-
- Main EK, Menard MK. Maternal mortality: time for national action. Obstet Gynecol 2013;122:735–6. - PubMed
-
- Main EK. Reducing Maternal Mortality and Severe Maternal Morbidity Through State-based Quality Improvement Initiatives. Clin Obstet Gynecol 2018;61:319–31. - PubMed
-
- D’Alton ME, Main EK, Menard MK, Levy BS. The National Partnership for Maternal Safety. Obstet Gynecol 2014;123:973–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
