

Clinical sign and biomarker-based algorithm to identify bacterial pneumonia among outpatients with lower respiratory tract infection in Tanzania
- PMID: 34991507
- PMCID: PMC8735728
- DOI: 10.1186/s12879-021-06994-9
Clinical sign and biomarker-based algorithm to identify bacterial pneumonia among outpatients with lower respiratory tract infection in Tanzania
Abstract
Background: Inappropriate antibiotics use in lower respiratory tract infections (LRTI) is a major contributor to resistance. We aimed to design an algorithm based on clinical signs and host biomarkers to identify bacterial community-acquired pneumonia (CAP) among patients with LRTI.
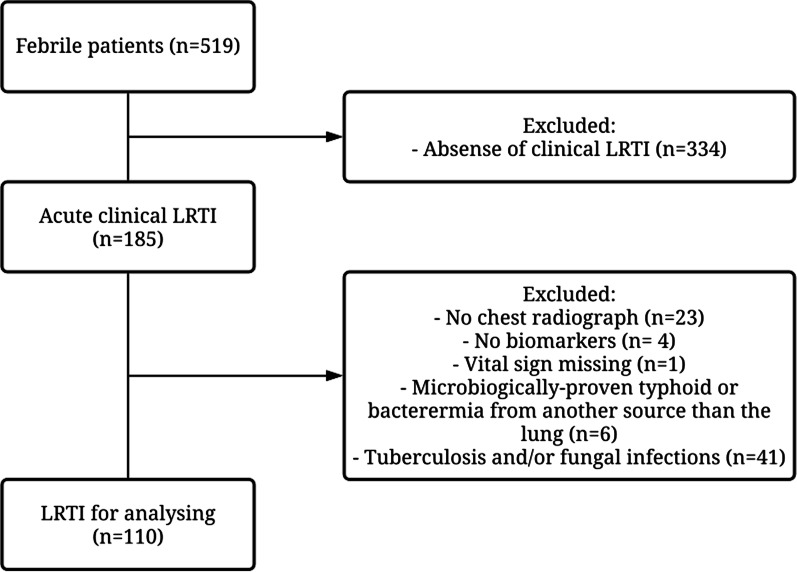
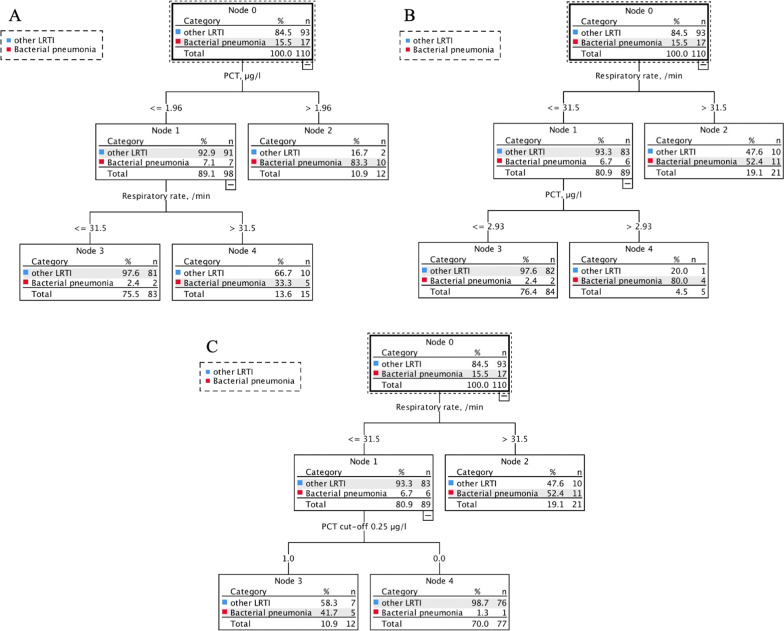
Methods: Participants with LRTI were selected in a prospective cohort of febrile (≥ 38 °C) adults presenting to outpatient clinics in Dar es Salaam. Participants underwent chest X-ray, multiplex PCR for respiratory pathogens, and measurements of 13 biomarkers. We evaluated the predictive accuracy of clinical signs and biomarkers using logistic regression and classification and regression tree analysis.
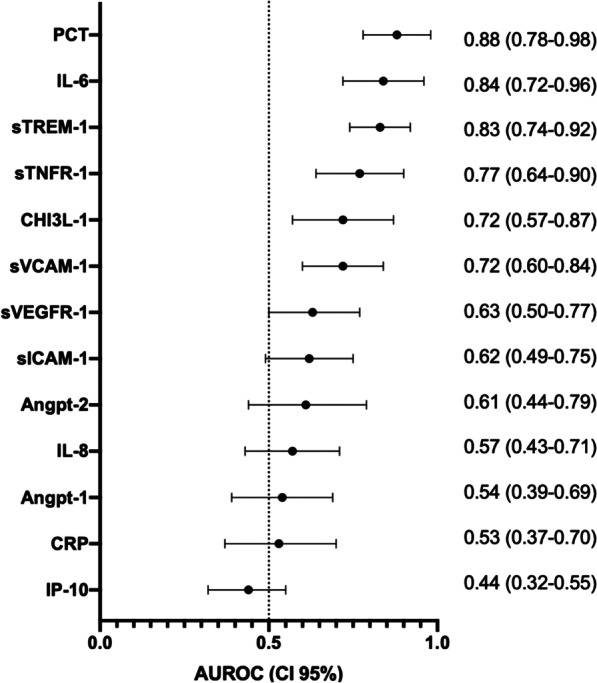
Results: Of 110 patients with LRTI, 17 had bacterial CAP. Procalcitonin (PCT), interleukin-6 (IL-6) and soluble triggering receptor expressed by myeloid cells-1 (sTREM-1) showed an excellent predictive accuracy to identify bacterial CAP (AUROC 0.88, 95%CI 0.78-0.98; 0.84, 0.72-0.99; 0.83, 0.74-0.92, respectively). Combining respiratory rate with PCT or IL-6 significantly improved the model compared to respiratory rate alone (p = 0.006, p = 0.033, respectively). An algorithm with respiratory rate (≥ 32/min) and PCT (≥ 0.25 μg/L) had 94% sensitivity and 82% specificity.
Conclusions: PCT, IL-6 and sTREM-1 had an excellent predictive accuracy in differentiating bacterial CAP from other LRTIs. An algorithm combining respiratory rate and PCT displayed even better performance in this sub-Sahara African setting.
Keywords: Bacterial community-acquired pneumonia; Biomarkers; PCT; Predicting algorithm.
© 2022. The Author(s).
Conflict of interest statement
All authors declare to have no conflict of interest.
Figures


References
-
- Bryan-Wilson J. No time to wait. Artforum Int. 2016;54(10):113–114.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
