

Military traumatic brain injury: a challenge straddling neurology and psychiatry
- PMID: 34991734
- PMCID: PMC8740337
- DOI: 10.1186/s40779-021-00363-y
Military traumatic brain injury: a challenge straddling neurology and psychiatry
Abstract
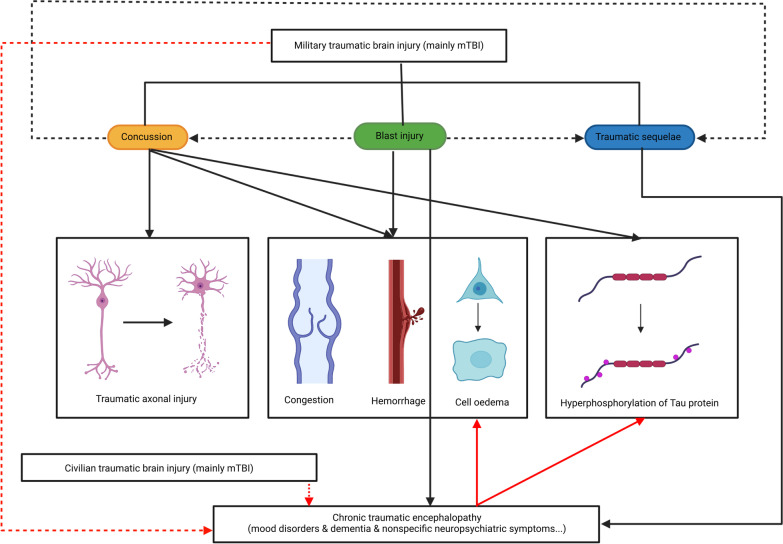
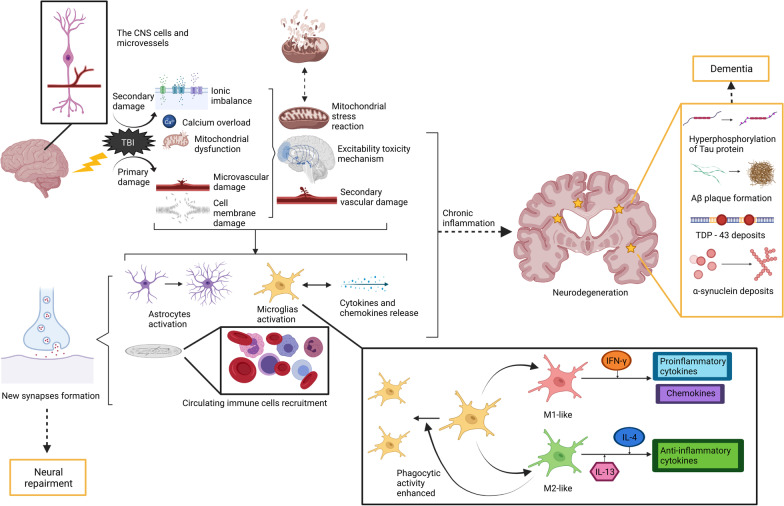
Military psychiatry, a new subcategory of psychiatry, has become an invaluable, intangible effect of the war. In this review, we begin by examining related military research, summarizing the related epidemiological data, neuropathology, and the research achievements of diagnosis and treatment technology, and discussing its comorbidity and sequelae. To date, advances in neuroimaging and molecular biology have greatly boosted the studies on military traumatic brain injury (TBI). In particular, in terms of pathophysiological mechanisms, several preclinical studies have identified abnormal protein accumulation, blood-brain barrier damage, and brain metabolism abnormalities involved in the development of TBI. As an important concept in the field of psychiatry, TBI is based on organic injury, which is largely different from many other mental disorders. Therefore, military TBI is both neuropathic and psychopathic, and is an emerging challenge at the intersection of neurology and psychiatry.
Keywords: Comorbidity; Diagnosis; Military; Shellshock; Traumatic brain injury; Treatment.
© 2022. The Author(s).
Conflict of interest statement
The authors have no competing interests to declare.
Figures
References
-
- Myers CS. A contribution to the study of shell shock. Lancet. 1915;185(4772):316–320.
-
- Mott FW. The effects of high explosives upon the central nervous system. Lancet. 1916;187(4824):331–338.
-
- Battle casualties: incidence, mortality, and logistic considerations. JAMA. 1952;150(13):1357.
-
- Hs M. Punch drunk. JAMA. 1928;91:1103–1107.
-
- Johnson J. Organic psychosyndromes due to boxing. Br J Psychiatry. 1969;115(518):45–53. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
