

Clinical research challenges posed by difficult-to-treat depression
- PMID: 34991768
- PMCID: PMC8883824
- DOI: 10.1017/S0033291721004943
Clinical research challenges posed by difficult-to-treat depression
Abstract
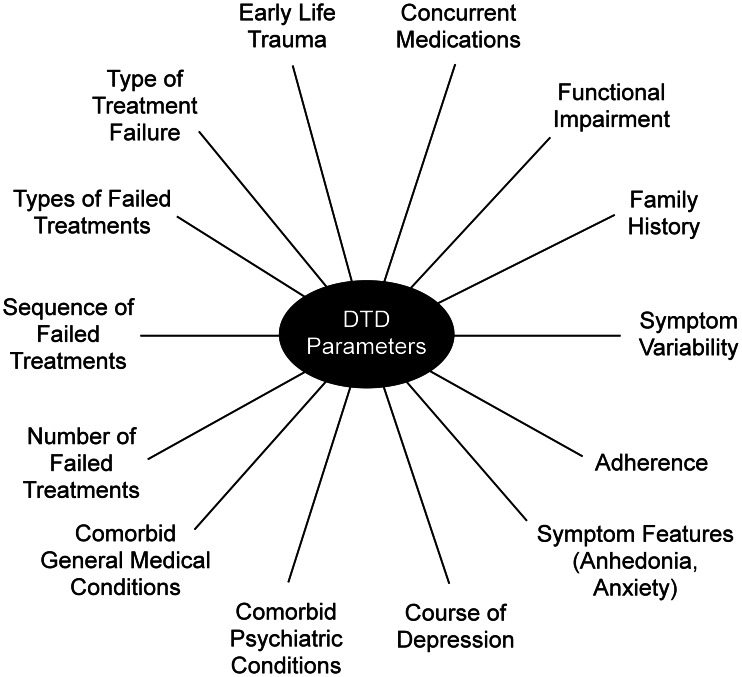
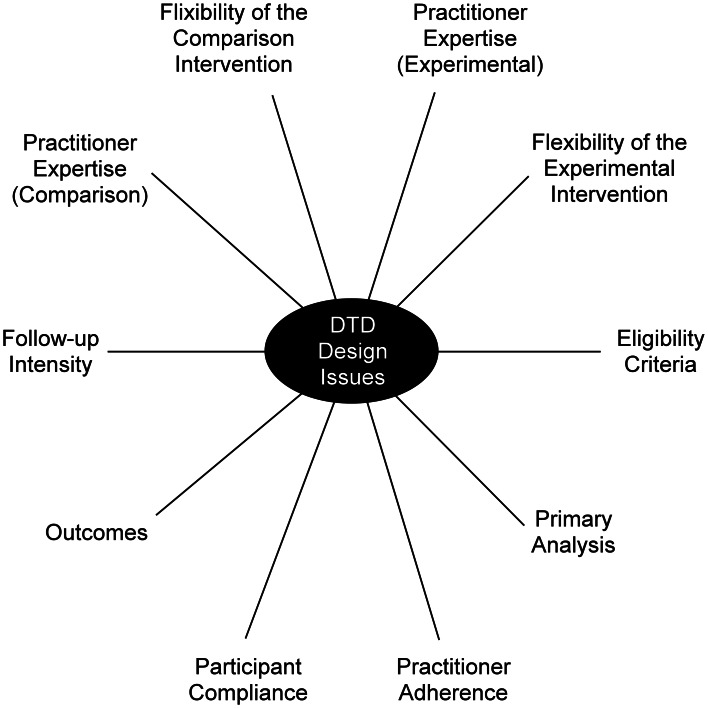
Approximately one-third of individuals in a major depressive episode will not achieve sustained remission despite multiple, well-delivered treatments. These patients experience prolonged suffering and disproportionately utilize mental and general health care resources. The recently proposed clinical heuristic of 'difficult-to-treat depression' (DTD) aims to broaden our understanding and focus attention on the identification, clinical management, treatment selection, and outcomes of such individuals. Clinical trial methodologies developed to detect short-term therapeutic effects in treatment-responsive populations may not be appropriate in DTD. This report reviews three essential challenges for clinical intervention research in DTD: (1) how to define and subtype this heterogeneous group of patients; (2) how, when, and by what methods to select, acquire, compile, and interpret clinically meaningful outcome metrics; and (3) how to choose among alternative clinical trial design options to promote causal inference and generalizability. The boundaries of DTD are uncertain, and an evidence-based taxonomy and reliable assessment tools are preconditions for clinical research and subtyping. Traditional outcome metrics in treatment-responsive depression may not apply to DTD, as they largely reflect the only short-term symptomatic change and do not incorporate durability of benefit, side effect burden, or sustained impact on quality of life or daily function. The trial methodology will also require modification as trials will likely be of longer duration to examine the sustained impact, raising complex issues regarding control group selection, blinding and its integrity, and concomitant treatments.
Keywords: Classification; difficult-to-treat depression; outcome measures; study design; taxonomy; treatment-resistant depression.
Conflict of interest statement
Dr Rush has received consulting fees from Compass Inc., Curbstone Consultant LLC, Emmes Corp., Evecxia Therapeutics, Inc., Holmusk, Johnson and Johnson (Janssen), LivaNova PLC, Neurocrine Biosciences Inc., Otsuka-US, Sunovion; speaking fees from LivaNova, Johnson and Johnson (Janssen); and royalties from Guilford Press and the University of Texas Southwestern Medical Center, Dallas, TX (for the Inventory of Depressive Symptoms and its derivatives). He is also named co-inventor on two patents: U.S. Patent No. 7 795 033: Methods to Predict the Outcome of Treatment with Antidepressant Medication, Inventors: McMahon FJ, Laje G, Manji H, Rush AJ, Paddock S, Wilson AS; and U.S. Patent No. 7 906 283: Methods to Identify Patients at Risk of Developing Adverse Events During Treatment with Antidepressant Medication, Inventors: McMahon FJ, Laje G, Manji H, Rush AJ, Paddock S. Dr Sackeim serves as a scientific adviser to Cerebral Therapeutics Inc., LivaNova PLC, MECTA Corporation, Neurolief Ltd., Neuronetics Inc, and Parow Entheobiosciences LLC. He receives honoraria and royalties from Elsevier Inc. and Oxford University Press. He is the inventor on non-remunerative US patents for Focal Electrically Administered Seizure Therapy (FEAST), titration in the current domain in ECT, and the adjustment of current in ECT devices, each held by the MECTA Corporation. He is also the originator of magnetic seizure therapy (MST). Dr Conway has received research support from Bristol-Myers Squibb, the Stanley Medical Research Institute, the National Institute of Mental Health, NeoSync, LivaNova PLC, the Taylor Family Institute for Innovative Psychiatric Research, the American Foundation for Suicide Prevention, Assurex Health Inc., August Busch IV Foundation, and Barnes-Jewish Hospital Foundation. He is a part-time employee at the John Cochran VA Medical Center in St. Louis. Dr Bunker is a former employee and a current consultant of LivaNova USA PLC. Dr Hollon has no disclosures. Dr Demyttenaere has received an honorarium for attending advisory boards, acting as a consultant or being a member of the speaker bureau for Boehringer-Ingelheim, Gedeon-Richter, Johnson and Johnson, LivaNova, Lundbeck, Pfizer and Recordati. Dr Young has received payment for lectures and advisory boards for the following companies: Astrazenaca, Eli Lilly, Lundbeck, Sunovion, Servier, LivaNova, Janssen, Allegan, Bionomics, Sumitomo Dainippon Pharma, COMPASS. He is a consultant to Johnson & Johnson and LivaNova. He has received honoraria for attending advisory boards and presenting talks at meetings organized by LivaNova. He is a Principal Investigator on studies funded by LivaNova; Janssen, COMPASS and Chief Investigator on a study funded by Novartis. He does not hold shares in pharmaceutical companies. Dr Aaronson is a consultant to Neuronetics, LivaNova, Janssen, Sage Therapeutics and Genomind. He also receives research support from Compass Pathways and Neuronetics. Dr Dibué is an employee of LivaNova PLC, a manufacturer of vagus nerve stimulators and holds stock options. Dr Thase reports the following relationships: Advisory/Consultant: Acadia, Inc., Akili, Inc., Alkermes PLC, Allergan, Inc., Clexio, H. Lundbeck, A/S, Jazz Pharmaceuticals, Johnson & Johnson (Janssen), Merck & Company, Inc., Otsuka Pharmaceutical Company, Ltd., Pfizer, Inc., and Seelos. Grant Support: Acadia, Inc., Allergan, Inc., AssureRx (now Myriad), Axsome Therapeutics Inc., Intracellular, Inc., Johnson & Johnson (Janssen), Otsuka Pharmaceutical Company, Ltd., Patient-Centered Outcomes Research Institute (PCORI), Takeda. Royalties: American Psychiatric Press, Guilford Publications, W.W. Norton & Company, Inc., and Wolters Kluwer. Spouse's Employment: Dr McAllister-Williams has received fees from American Center for Psychiatry & Neurology, United Arab Emirates, British Association for Psychopharmacology, European College of Neuropsychopharmacology, International Society for Affective Disorders, Janssen, LivaNova, Lundbeck, My Tomorrows, OCM Comunicaziona s.n.c., Pfizer, Qatar International Mental Health Conference, Sunovion, Syntropharma, UK Medical Research Council and Wiley; grant support from National Institute for Health Research Efficacy and Mechanism Evaluation Panel and Health Technology Assessment Panel; and non-financial support from COMPASS Pathways and Magstim.
Figures

References
-
- Aaronson, S. T., Sears, P., Ruvuna, F., Bunker, M., Conway, C. R., Dougherty, D. D., … Zajecka, J. M. (2017). A 5-year observational study of patients with treatment-resistant depression treated with vagus nerve stimulation or treatment as usual: Comparison of response, remission, and suicidality. American Journal of Psychiatry, 174, 640–648. doi: 10.1176/appi.ajp.2017 - DOI - PubMed
-
- Agency for Healthcare Research and Policy (AHQR) (Sept 2011). Nonpharmacologic interventions for treatment-resistant depression in adults (comparative effectiveness review number 33). Rockville, MD: AHQR.
-
- Amital, D., Fostick, L., Silberman, A., Calati, R., Spindelegger, C., Serretti, A., … Zohar, J. (2013). Physical co-morbidity among treatment-resistant vs. treatment responsive patients with major depressive disorder. European Neuropsychopharmacology, 23, 895–901. doi: 10.1016/j.euroneuro.2012.09.002 - DOI - PubMed
-
- Amos, T. B., Tandon, N., Lefebvre, P., Pilon, D., Kamstra, R. L., Pivneva, I., & Greenberg, P. E. (2018). Direct and indirect cost burden and change of employment status in treatment-resistant depression: A matched cohort study using a US commercial claims database. Journal of Clinical Psychiatry, 79(2), 17m11725. doi: 10.4088/JCP.17m11725 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
