

Does adherence to a quality indicator regarding early weaning from invasive ventilation improve economic outcome? A single-centre retrospective study
- PMID: 34992097
- PMCID: PMC8739420
- DOI: 10.1136/bmjopen-2020-045327
Does adherence to a quality indicator regarding early weaning from invasive ventilation improve economic outcome? A single-centre retrospective study
Abstract
Objectives: To measure and assess the economic impact of adherence to a single quality indicator (QI) regarding weaning from invasive ventilation.
Design: Retrospective observational single-centre study, based on electronic medical and administrative records.
Setting: Intensive care unit (ICU) of a German university hospital, reference centre for acute respiratory distress syndrome.
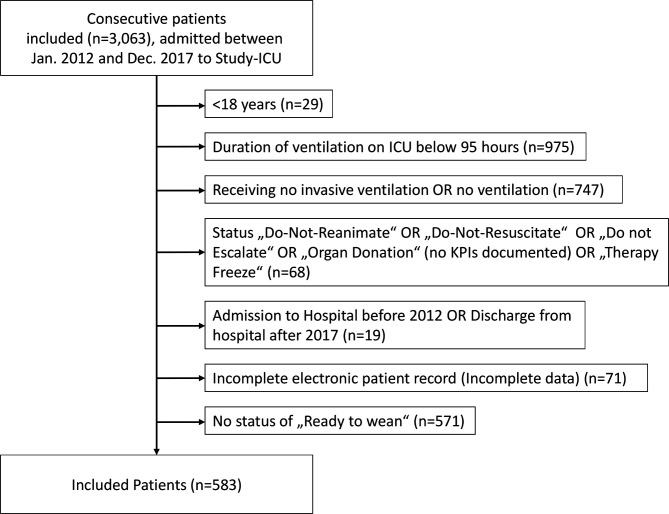
Participants: Records of 3063 consecutive mechanically ventilated patients admitted to the ICU between 2012 and 2017 were extracted, of whom 583 were eligible adults for further analysis. Patients' weaning protocols were evaluated for daily adherence to quality standards until ICU discharge. Patients with <65% compliance were assigned to the low adherence group (LAG), patients with ≥65% to the high adherence group (HAG).
Primary and secondary outcome measures: Economic healthcare costs, clinical outcomes and patients' characteristics.
Results: The LAG consisted of 378 patients with a median negative economic results of -€3969, HAG of 205 (-€1030), respectively (p<0.001). Median duration of ventilation was 476 (248; 769) hours in the LAG and 389 (247; 608) hours in the HAG (p<0.001). Length of stay (LOS) in the LAG on ICU was 21 (12; 35) days and 16 (11; 25) days in the HAG (p<0.001). LOS in the hospital was 36 (22; 61) days in the LAG, and within the HAG, respectively, 26 (18; 48) days (p=0.001).
Conclusions: High adherence to this single QI is associated with better clinical outcome and improved economic returns. Therefore, the results support the adherence to QI. However, the examined QI does not influence economic outcome as the decisive factor.
Keywords: health economics; intensive & critical care; quality in health care.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: CS reports grants from Aridis Pharmaceutical, grants from B. Braun Melsungen AG, grants from Drägerwerk AG & Co. KGaA, grants from Deutsche Forschungsgemeinschaft/German Research Society, grants from Deutsches Zentrum für Luft- und Raumfahrt e. V. (DLR)/German Aerospace Centre, grants from Einstein Stiftung Berlin/Einstein Foundation Berlin, grants from European Society of Anaesthesiology, grants from Gemeinsamer Bundesausschuss/Federal Joint Committee (G-BA), grants from Inneruniversitäre Forschungsförderung/Inner University Grants, grants from Projektträger im DLR/Project Management Agency, grants from Stifterverband/Non-Profit Society Promoting Science and Education, grants from WHOCC, grants from Baxter Deutschland, grants from Cytosorbents Europe, grants from Edwards Lifesciences Germany, grants from Fresenius Medical Care, grants from Grünenthal, grants from Masimo Europe, grants from Pfizer Pharma PFE, personal fees from Georg Thieme Verlag, grants from Dr. F. Köhler Chemie, grants from Sintetica, grants from European Commission, grants from Stifterverband für die deutsche Wissenschaft e.V./Philips, grants from Stiftung Charité, grants from AGUETTANT Deutschland, grants from AbbVie Deutschland GmbH & Co. KG, grants from Amomed Pharma GmbH, grants from InTouch Health, grants from Copra System, grants from Correvio, grants from Max-Planck-Gesellschaft zur Förderung der Wissenschaften e.V., grants from Deutsche Gesellschaft für Anästhesiologie & Intensivmeidzin (DGAI), grants from Stifterverband für die deutsche Wissenschaft e.V./Medtronic, grants from Philips Electronics Nederland BV, grants from BMH, outside the submitted work; In addition, CS has a patent 10 2014 215 211.9 licensed, a patent 10 2014 215 212.9 licensed, a patent 10 2018 114 364.8 licensed, and a patent 10 2018 110 275.5 licensed. MH has nothing to disclose. MD has nothing to disclose. RA has nothing to disclose. JK has nothing to disclose. RJ has nothing to disclose. FB reports grants from Einstein Foundation, personal fees from Axon Publishing, grants from Vifor Pharma, personal fees from Elsevier Publishing, grants from Federal Ministry of Health, Germany, grants from Berlin Institute of Health, outside the submitted work.
Figures
References
-
- Cooper LM, Linde-Zwirble WT. Medicare intensive care unit use: analysis of incidence, cost, and payment. Crit Care Med 2004;32:2247–53. 10.1097/01.CCM.0000146301.47334.BD - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources