

A national evaluation of geographic accessibility and provider availability of obesity medicine diplomates in the United States between 2011 and 2019
- PMID: 34992242
- PMCID: PMC8881297
- DOI: 10.1038/s41366-021-01024-9
A national evaluation of geographic accessibility and provider availability of obesity medicine diplomates in the United States between 2011 and 2019
Abstract
Background/objectives: Obesity is a pressing health concern within the United States (US). Obesity medicine "diplomates" receive specialized training, yet it is unclear if their accessibility and availability adequately serves the need. The purpose of this research was to understand how accessibility has evolved over time and assess the practicality of serving an estimated patient population with the current distribution and quantity of diplomates.
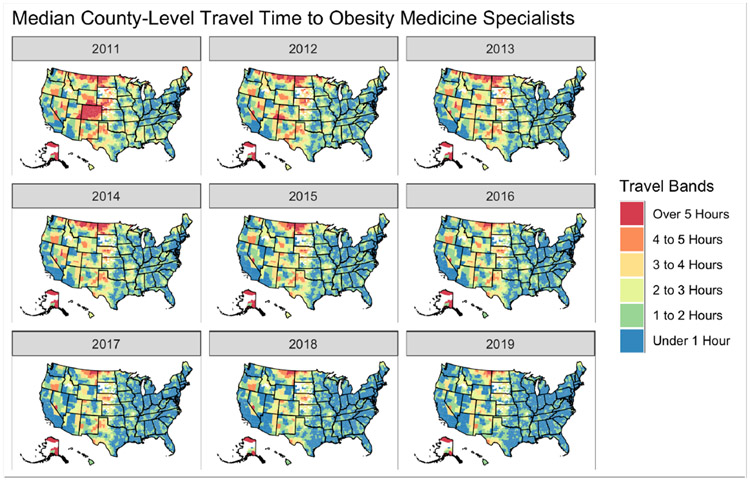
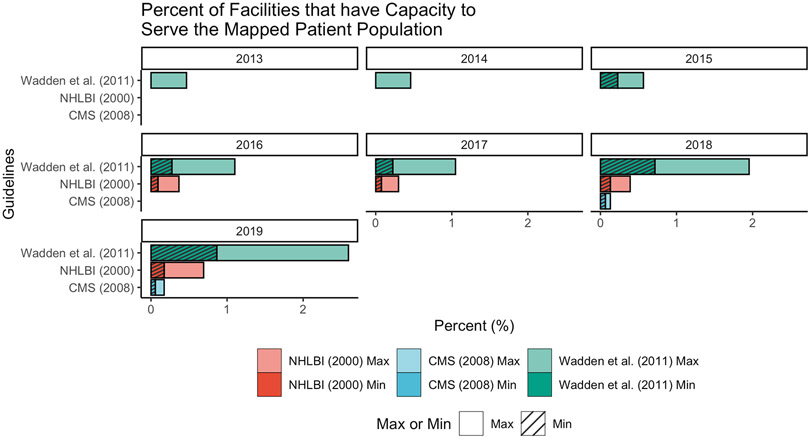
Methods: Population-weighted Census tracts in US counties were mapped to the nearest facility on a road network with at least one diplomate who specialized in adult (including geriatric) care between 2011 and 2019. The median travel time for all Census tracts within a county represented the primary geographic access measure. Availability was assessed by estimating the number of diplomates per 100 000 patients with obesity and the number of facilities able to serve assigned patients under three clinical guidelines.
Results: Of the 3371 diplomates certified since 2019, 3036 were included. The median travel time (weighted for county population) fell from 28.5 min [IQR: 13.7, 68.1] in 2011 to 9.95 min [IQR: 7.49, 18.1] in 2019. There were distinct intra- and inter-year travel time variations by race, ethnicity, education, median household income, rurality, and Census region (all P < 0.001). The median number of diplomates per 100 000 with obesity grew from 1 [IQR: 0.39, 1.59] in 2011 to 5 [IQR: 2.74, 11.4] in 2019. In 2019, an estimated 1.7% of facilities could meet the recommended number of visits for all mapped patients with obesity, up from 0% in 2011.
Conclusions: Diplomate geographic access and availability have improved over time, yet there is still not a high enough supply to serve the potential patient demand. Future studies should quantify patient-level associations between travel time and health outcomes, including whether the number of available diplomates impacts utilization.
© 2021. The Author(s), under exclusive licence to Springer Nature Limited.
Figures
References
-
- Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of Obesity and Severe Obesity Among Adults: United States, 2017–2018. National Center for Health Statistics: Hyattsville, MD, 2020. https://www.cdc.gov/nchs/products/databriefs/db360.htm (accessed 5 Nov2020).
-
- Pischon T, Nöthlings U, Boeing H. Obesity and cancer. Proc Nutr Soc 2008; 67: 128–145. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
