

doi: 10.1016/j.jcot.2021.101724.
eCollection 2022 Feb.
Role of the Ilizarov fixator in high tibial osteotomy
Affiliations
- PMID: 34993051
- PMCID: PMC8704438
- DOI: 10.1016/j.jcot.2021.101724
Item in Clipboard
Role of the Ilizarov fixator in high tibial osteotomy
J Clin Orthop Trauma.
.
No abstract available
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
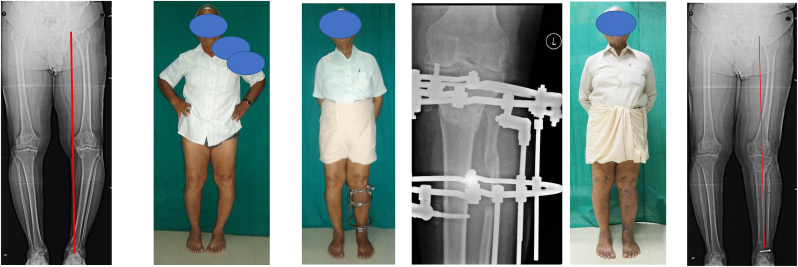
a, b. 70-year-old bodybuilder had a large varus deformity with intorsion of the tibia. The mechanical axis has deviated to less than 0%. c, d. A hybrid Ilizarov fixator with half-pin fixation was done. A proximal fibulectomy is necessary. A curved Focal Dome osteotomy with a distal convexity is performed. Proximal fixation is with one ring with a half-pin proximal and distal to the ring. A plain wire ensures parallelism to the joint. Distal fixation is with two rings and two half pins. Angulation is achieved with multi-plane hinges. More valgus can be achieved by compressing lateral struts. Uniform compression achieves better bony contact and reliable healing. e,f. accurate correction without causing overcorrection to enable the mechanical axis to pass just lateral to the midline. Has given lasting pain relief for more than seven years now.

a,b,c,d. 60-year-old lady had a large varus and FFD on the Right lower limb. e. The TSF fixator was used instead of the Ilizarov. Incisions of the fibulectomy and anterior incision for retinacular release with dome osteotomy are seen. Once the varus and procurvatum ( FFD) are corrected. A plate is inserted on the medial side. f,g,h. Full-length x-rays show good correction of the axis, also seen clinically. Close-up AP shows dome osteotomy with the minimal lateral translation of distal fragment. Lateral x-ray shows a reduction of the tibial slope to correct the FFD of the knee.
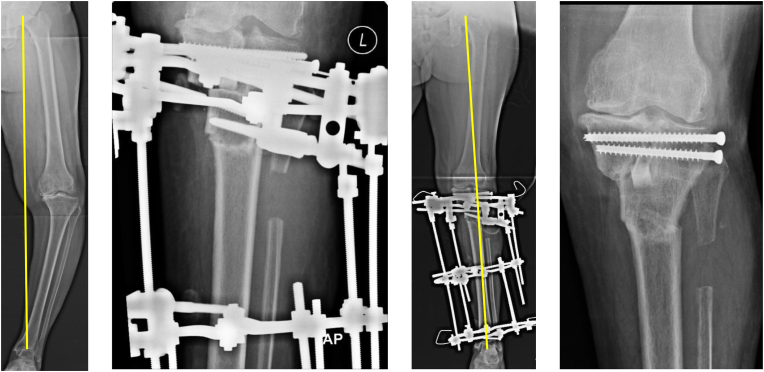
a,b,c,d. Large varus deformity with an obvious upper tibial extra-articular deformity and also a “pagoda tibia” showing an intra-articular deformity. Ilizarov fixator was used to fix the double osteotomy. The Upper osteotomy is an L-shaped osteotomy with elevation of medial tibial condyle. This is fixed with two Cancellous screws. This improves the congruity of the articular contact. The gap is filled with an excised piece of the fibula. The upper osteotomy zone is also fixed with two half-pins. 4 cm intervening zone had a fixation with two half pins. All these four pins are fixed to the upper ring. A Distal dome osteotomy is performed with the lateral translation of distal fragment which allows adequate correction of mechanical axis ( seen on intra-operative x-rays).
References
-
- Paley D. In: Arthritis and Arthroplasty: The Knee. Brown T.E., Cui Q., Mihalko W., Saleh K., editors. W.B. Saunders.; Philadelphia: 2004. Principles of correction for monocompartmental arthritis of the knee; pp. 37–61.
-
- Fujisawa Y., Masuhara K., Shiomi S. The effect of high tibial osteotomy on osteoarthritis of the knee. An arthroscopic study of 54 knee joints. Orthop Clin N Am. 1979;10(3):585–608. - PubMed
-
- Paley D. In: Principles of Deformity Correction. Herzenberg J.E., editor. Springer/Berlin Heidelberg; 2005. Realigment for mono-compartment osteoarthritis of knee; pp. 479–507.
-
- Christodoulou N.A., Tsaknis R.N., Sdrenias C.V., Galanis K.G., Mavrogenis A.F. Improvement of proximal tibial osteotomy results by lateral retinacular release. Clin Orthop Relat Res. 2005;441:340–345. - PubMed
-
- Koshino T., Saito T., Orito K., Mitsuhashi S., Takeuchi R., Kurosaka T. Increase in range of knee motion to obtain floor sitting after high tibial osteotomy for osteoarthritis. Knee. 2002;9(3):189–196. - PubMed
LinkOut - more resources
Full Text Sources